Slipped Rib Syndrome
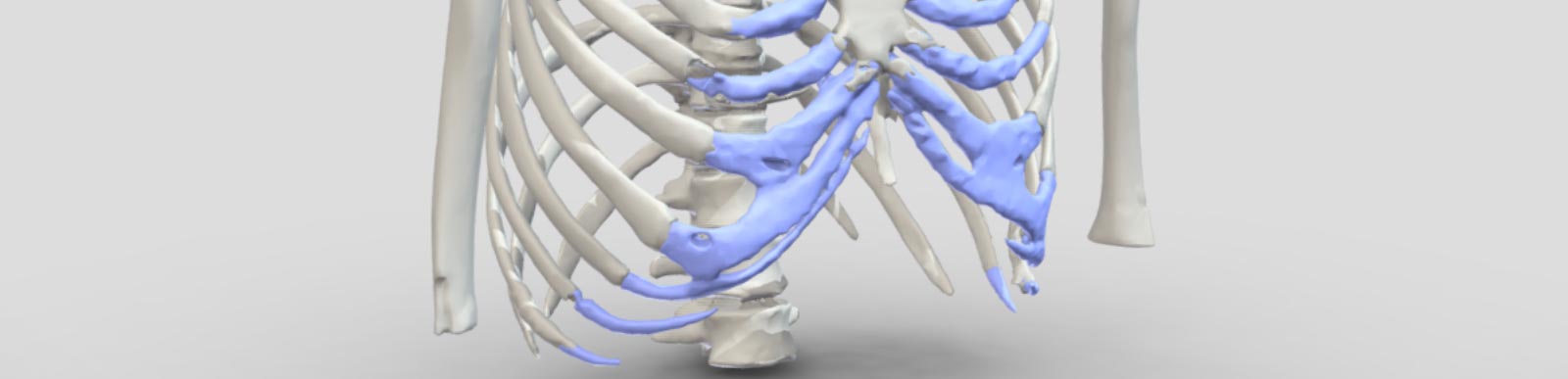
Slipped rib syndrome was first described in the early 1900’s by Cyriax and is an underdiagnosed and often poorly understand condition of the costal arch or margin. It's caused by excessive movement of the anterior cartilaginous part of the lower ribs as they ‘join’ the costal arch. The excessive movement or hypermobility of the anterior part of the ribs, typically the 8th, 9th or 10th rib is probably caused by either congenital or acquired (following a minor injury or repetitive strain) disruption of the fibrous junctions of these 'false' ribs at the costal arch, allowing the tips of the ribs to move or slip under the rib above. The movement causes lower rib or upper abdominal pain.
Created for the Rib Injury Clinic by AnatomikModeling
Symptoms
The pain is caused by excessive movement of the lower rib tips as they pass under the costal arch (what is sometimes called subluxing). It may be associated with a reported clicking or popping sensation. The pain is typically with certain movements or activities usually involving twisting, bending, deep breathing (so may come on after exercise) or even sneezing or coughing. The pain is often intermittent and sharp when the rib tip is moving excessively but can also be more like a dull ache particularly after an activity that 'triggers' movement. Resting, avoiding certain activities or even stretching out the rib cage can alleviate the pain.
Slipped rib syndrome tends to be one-sided though can affect both sides, tends to affect younger patients though any age can be affected and seems to be more common in certain sports or recreational activities such as swimming. Previous rib injury may lead to a form of acquired Slipped Rib Syndrome. Hypermobility and joint laxity also appear to be linked as does the presence of rib flare and other chest wall problems such as pectus deformities.
Investigations
Diagnosis of Slipped Rib Syndrome can often be difficult due to the nature of the pain and the many other chest or abdominal conditions that can cause pain in this part of the body. Seeing a doctor who is familiar with Slipped Rib Syndrome is important in assessing and investigating the condition. Clinical examination may relieve tenderness over the area and occasionally the hypermobile rib tip can be palpated and if moved can generate the pain (the hook Manoeuvre).
Patients may have had multiple investigations already and often Chest CT or even MRI tends not to be helpful. Dynamic Ultrasound with a radiologist experienced with Slipped Rib Syndrome is essential and often allows the radiologist to demonstrate excessive movement of the rib tip affected.
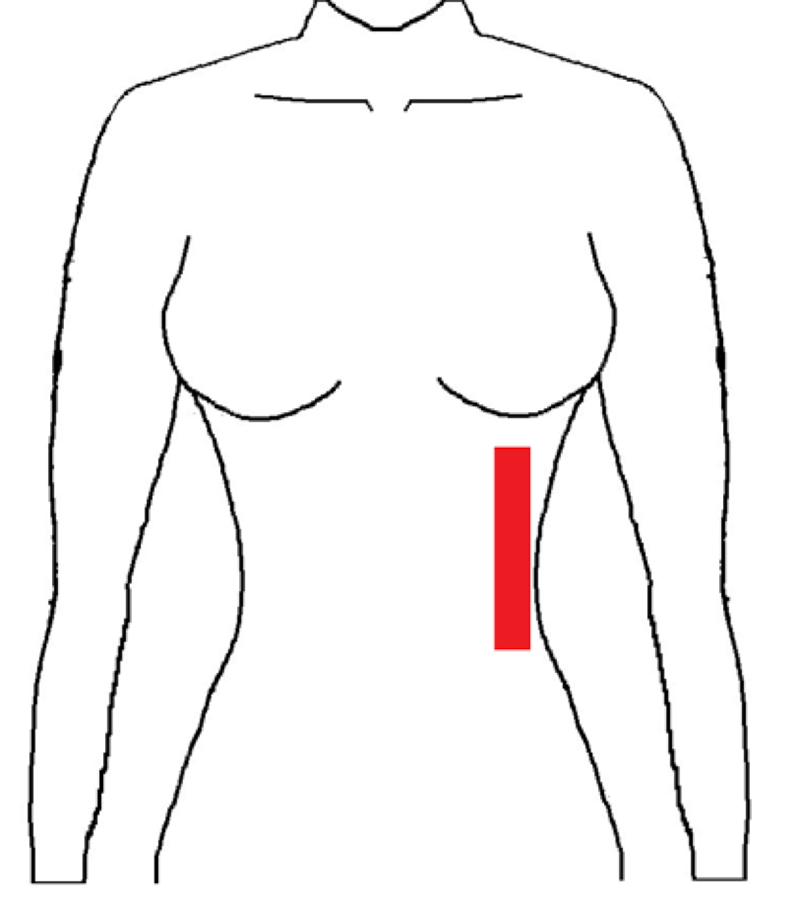
Probe position of Ultrasound
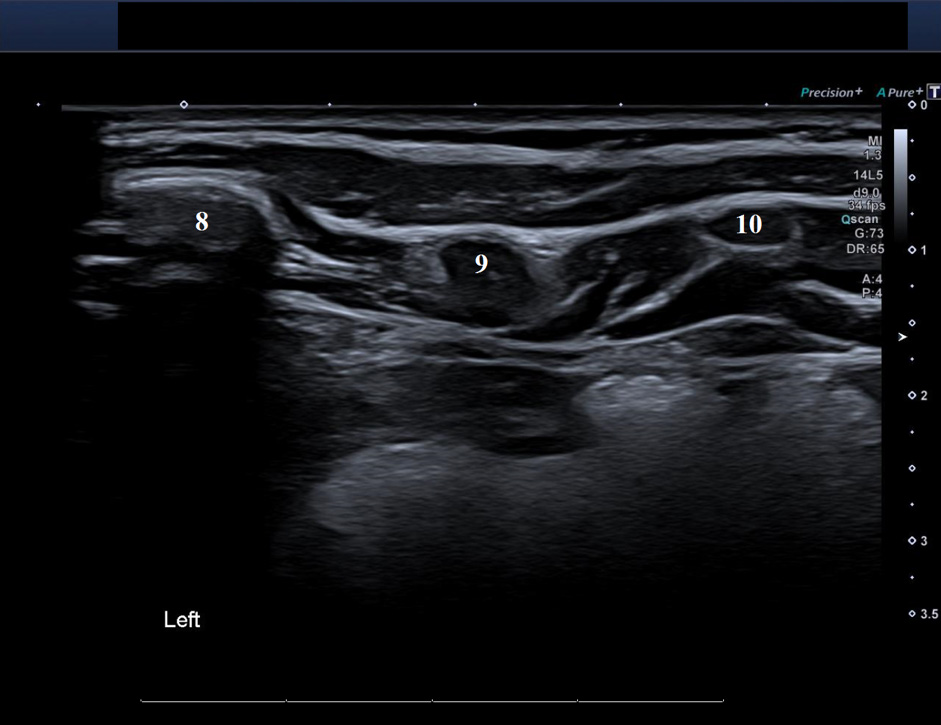
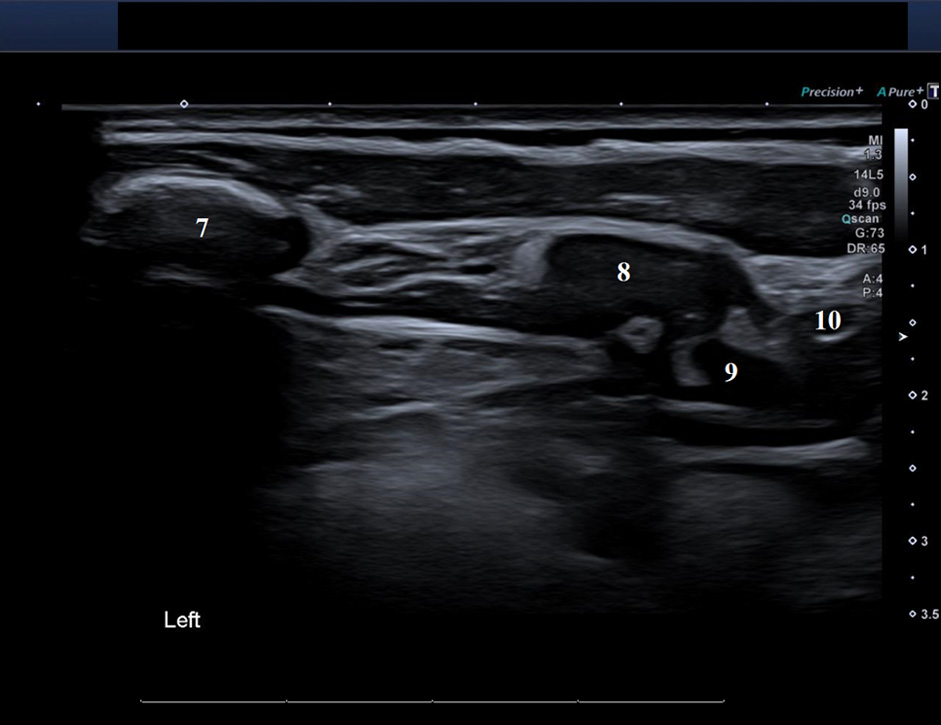
Ultrasound images with BEFORE [sliding] and AFTER following a dynamic movement (twisting) with pain. It demonstrates movement of the left 9th rib sliding under the adjacent ribs
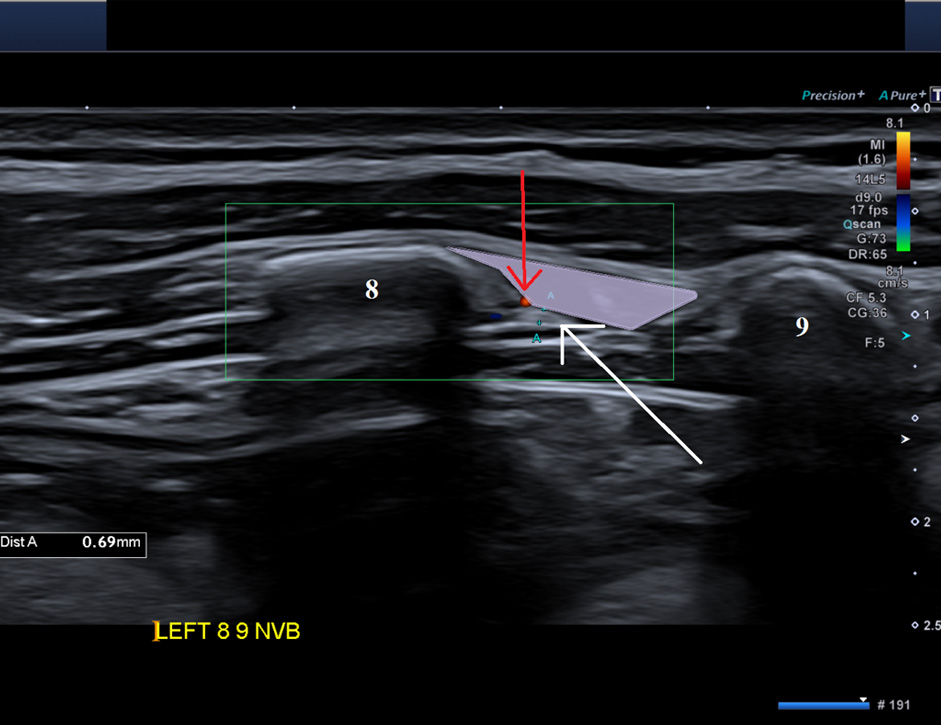
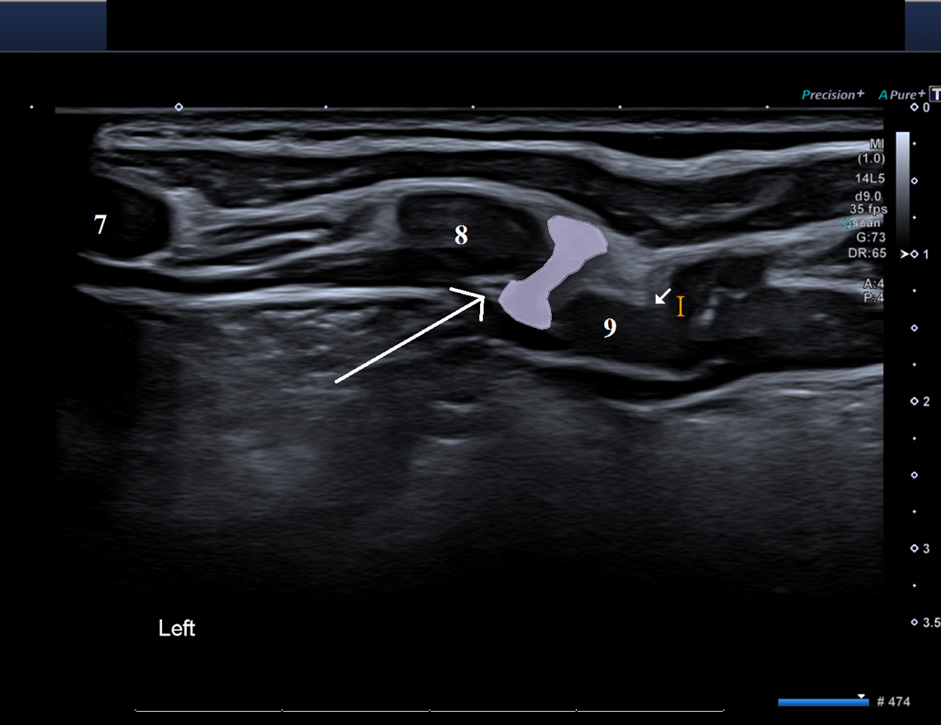
Ultrasound images of another patient demonstrating BEFORE (LEFT) and AFTER (RIGHT) following a dynamic movement (twisting) with generation of pain. The images demonstrate the 'distortion' of the intercostal muscle (shown in pink) due to excessive movement of the 9th rib. The long white arrow point to the nerve which is impinged by the muscle distortion. The red arrow is the artery.
Occasionally if the diagnosis is less clear cut, diagnostic local anaesthetic injection to the intercostal nerves corresponding to the rib tip involved can help confirm likely Slipping Rib Syndrome. Using Local anaesthetic block with or without corticosteroid may give temporary relief and occasionally complete relief of discomfort and can be considered as a potential treatment option.
Treatment
Establishing the diagnosis with a careful clinical history and examination together with a focused dynamic ultrasound scan allows a discussion with the patient different options and often a simple recognition and reassurance of the problem may be enough. Taking a conservative approach is acceptable once diagnosed and would include avoidance of activity aggravating pain, rest, NSAIDS and occasionally 'manipulative' physical therapy techniques may all help. If conservative treatment is not helping a trial of local anaesthetic with or without corticosteroid may be considered.
Surgery remains a good treatment with reports of excellent outcomes though recurrence of the pain has also been described. Typically, through a small targeted incision, the mobile rib tip is delivered from under the costal arch and excised. Alternately, the slipping rib can be stabilised to prevent slippage. See Surgery Treatment
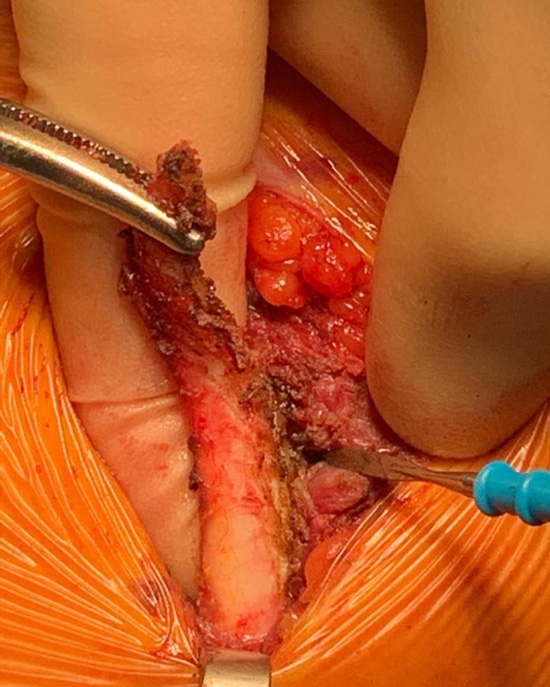
Intraoperative photo of excessively mobile rib tip that has been identified, grasped and mobilised from under the costal arch (in this case the tip of the left 10th rib)