Surgery
If non-surgical techniques fail to deal with chest wall problems, surgery may be necessary. The indication for chest wall surgery varies according to the problem but generally relates to persistent pain, deformity, occasionally symptoms of breathlessness and an inability to complete daily activities including sports and exercise.
Types of Surgery
The types of chest wall surgery can be broadly classified into:
1. Open reduction and internal fixation (ORIF)
Reduction of the fracture fragments back to normal anatomy and internally fixing, typically using purpose made metal plates, holding bone in place, often referred as chest wall stabilisation.
2. Excision of abnormal area or site of injury
Removal or separation of bony elements and prevention of mechanical rubbing and inflammation. Occasionally abnormal chest wall lumps may require removal through excision.
3. Repair and reconstruction of chest wall
Returning the contents of the chest cavity or chest wall itself to normal, for example repair of diagrammatic injury or reduction of lung hernia. Occasionally, if dealing with a chest wall tumour, removal (resection) of the tumour is carried out prior to repair and reconstruction.
All 3 approaches may be appropriate alone or occasionally in combination to deal with chest wall issues.
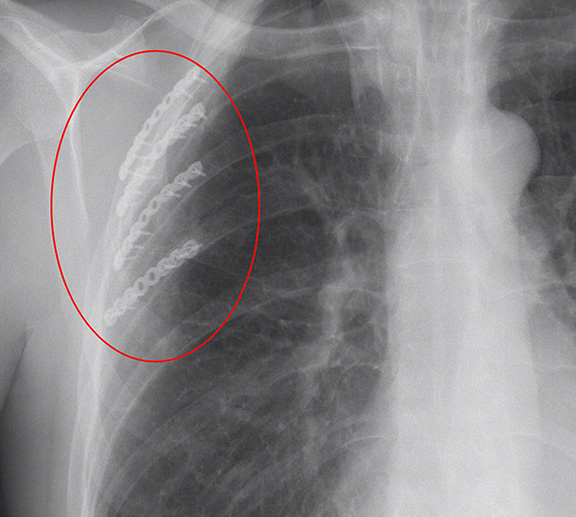
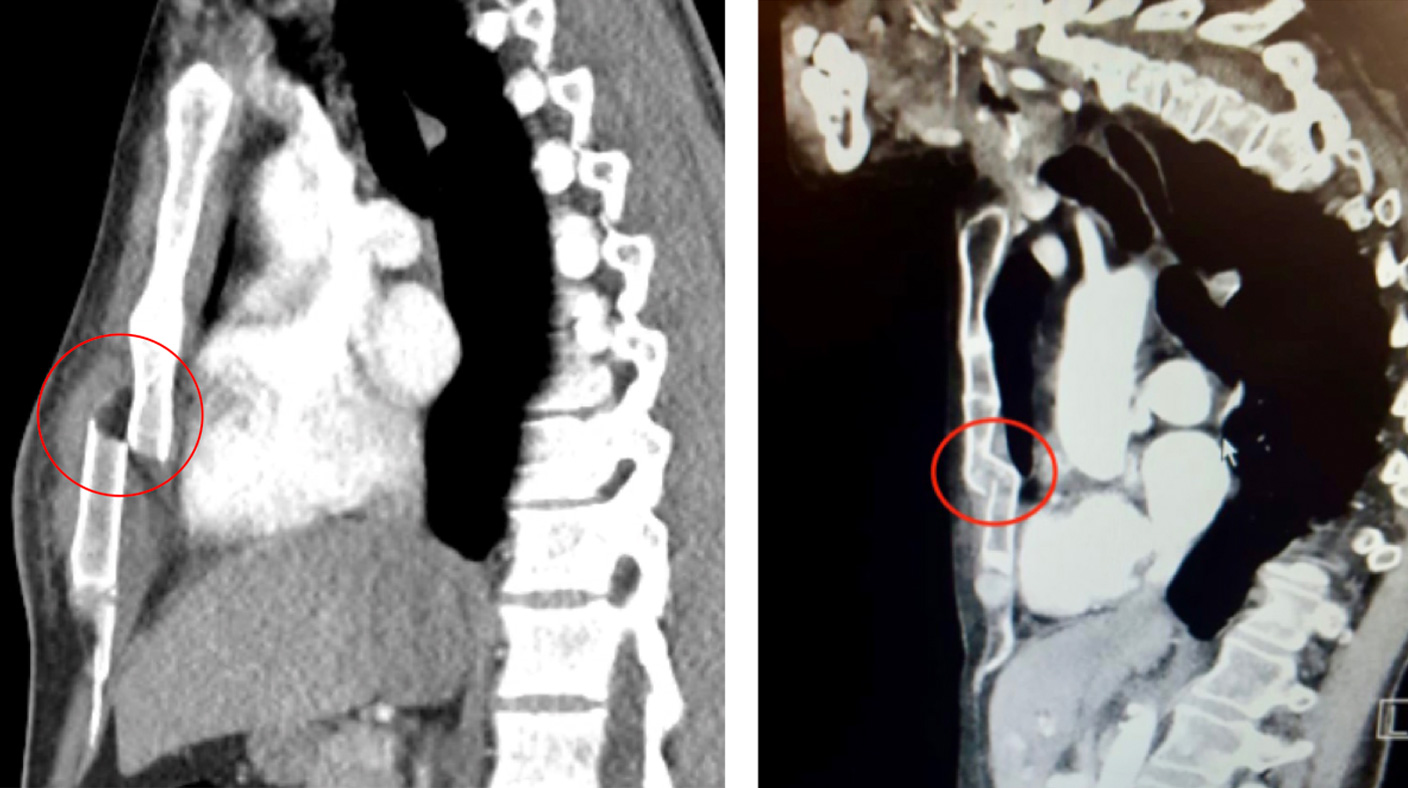
Open reduction and internal Rib fixation following a right chest wall injury and 4 rib fractures following fall downstairs (red ring).
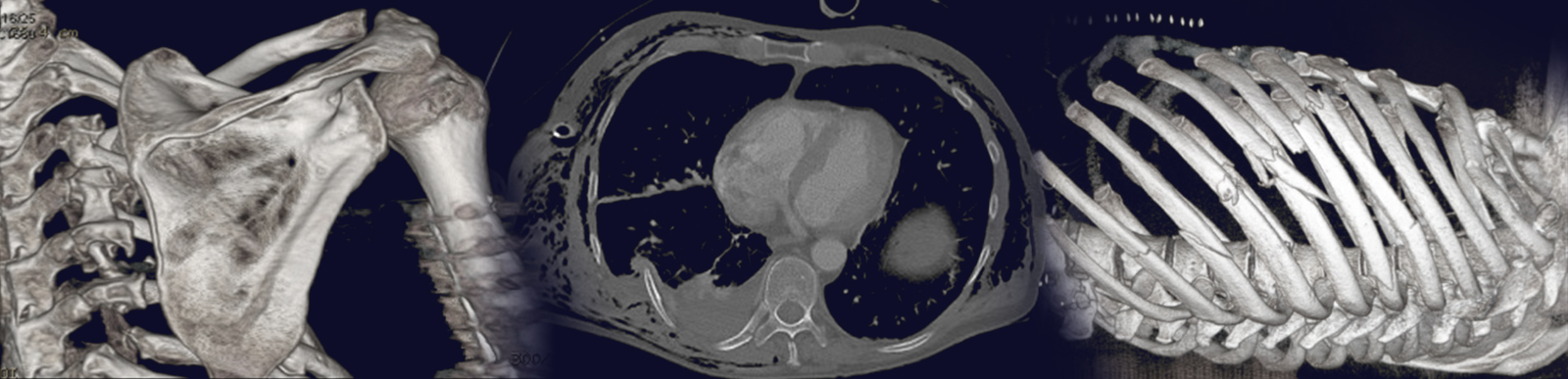
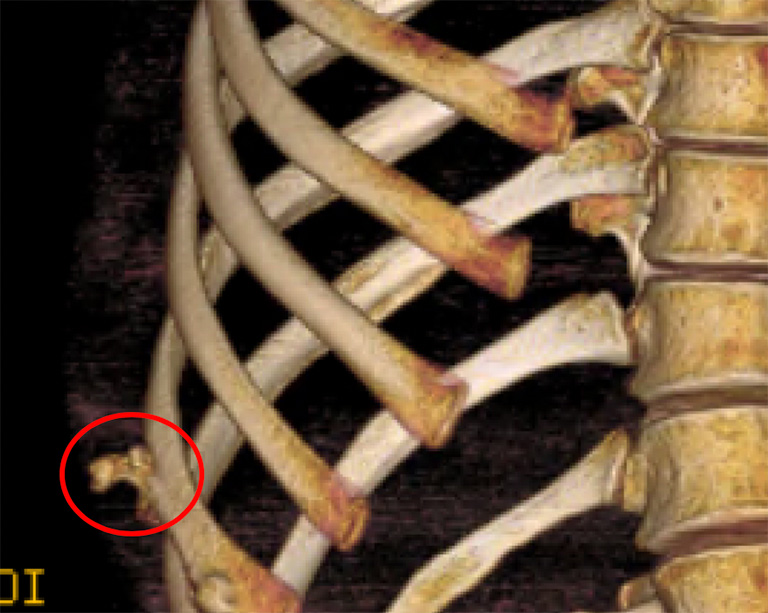
CT reconstruction chest in a patient with persistent and long-standing chest wall pain and tenderness at the site of an old poorly healed right 11th rib fracture (red ring). The painful area was excised and the pain resolved.
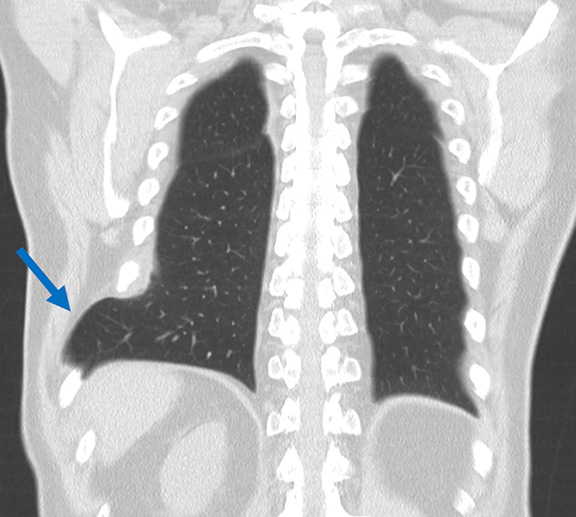
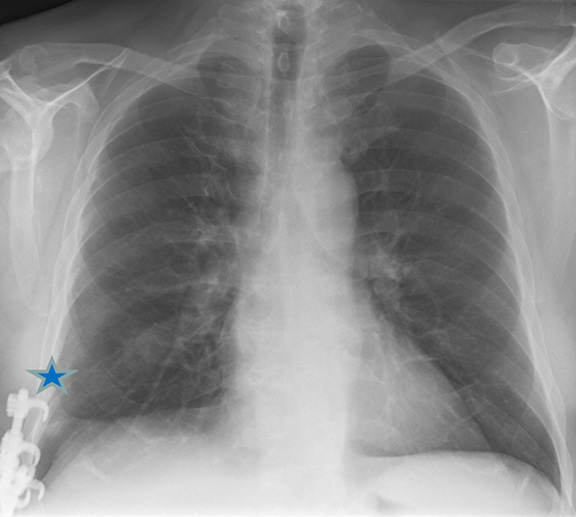
CT image showing chronic lung hernia (arrow) following rib injury (left) and Chest X-ray following Repair and reconstruction of chest wall with reduction of lung hernia and complex rib fixation (star).
Patient selection
The indications for surgical treatment for chest injuries include:
Pain: Usually acutely immediately and the first few days after the rib or sternal injury but if the bone fails to heal properly, the pain can become chronic and persistent. Rarely a problem with sternal injuries, chronic pain particularly with certain activities such as twisting, coughing or certain exercises is associated with specific complex chest wall injuries such as costochondral injuries or slipped rib syndrome.
Breathlessness: Immediately following the chest injury and in the first few days after the injury breathing issues are common and can be severe, requiring hospitalisation and breathing support such as oxygen. In most, however deep breathing hurts and coughing is difficult
Deformity: If the rib fractures are multiple (usually more than 3 ribs broken) and/or the ribs or sternum are badly displaced. Occasionally, in severe rib injuries with multiple breaks a ‘flail segment’ can develop where the chest wall moves paradoxically (moves inwards when breathing in when it should move out with the rest of the chest). One specific problem seen if the displayed rib fractures are under the arc of movement of the scapula or shoulder blade can lead to a ‘clunking’ sensation when the scapula is moved. With complex chest wall injuries, if a fracture dislocation heals badly it can lead to deformity and pain on movement.
Chest wall lump: A lump may be due to a poorly healed injury such as a fracture of the costal arch. If the abnormality is a lump on the chest wall, the indications are less related to symptoms (though pain and discomfort can be a problem) but may relate to concerns about malignancy (cancer) and risks of growth. Occasionally the lump can be unsightly.
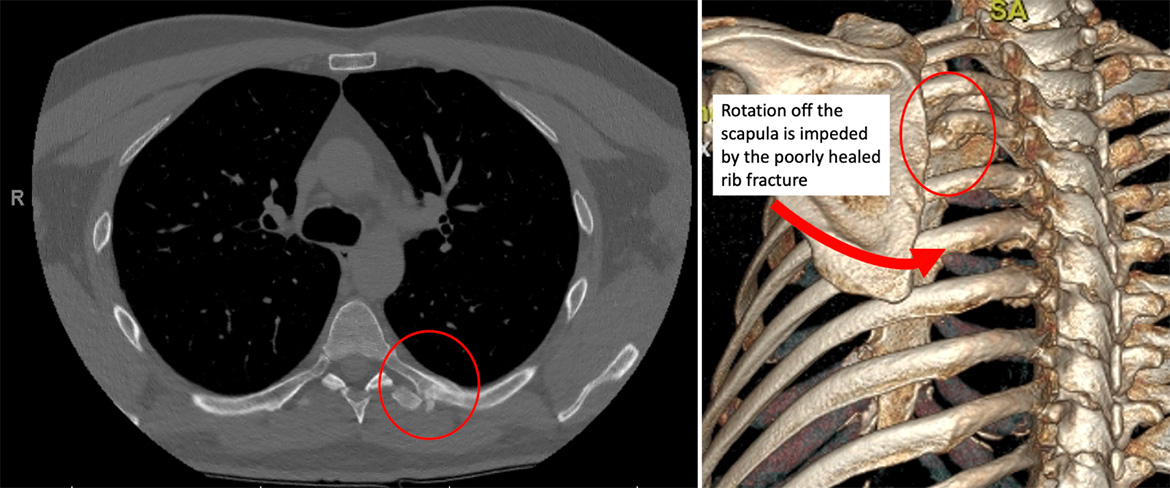
A poorly healed rib fracture (left, red ring) can lead to deformity and affect movement. In this case the patient complained of pain and a ‘clunking’ sensation when moving his left shoulder (right).
Choice of operation
The choice of operation depends on several factors including chronicity (how old is the injury), severity of sternal or rib injury and number of rib fractures as well as location of injury such as costosternal or costochondral junction injury and symptom (pain, instability or deformity).
Open Reduction Internal fixation
The most common operation offered for Rib and sternal injuries and sometimes used for more complex chest wall injuries, Open Reduction Internal Fixation (ORIF) of ribs and sternum was first described decades ago but it took the development of the materials and ‘hardware’ for rib fixation to become standard surgical treatment for rib fractures.
Mr Hunt performs has a high volume thoracic surgical practice with many cases performed as a keyhole procedure or through small incisions.
For Rib injuries, following a general anaesthetics (asleep) a small hole is made (VATS, Video Assisted Thoracoscopic Surgery) to assess the chest (or pleural) cavity.
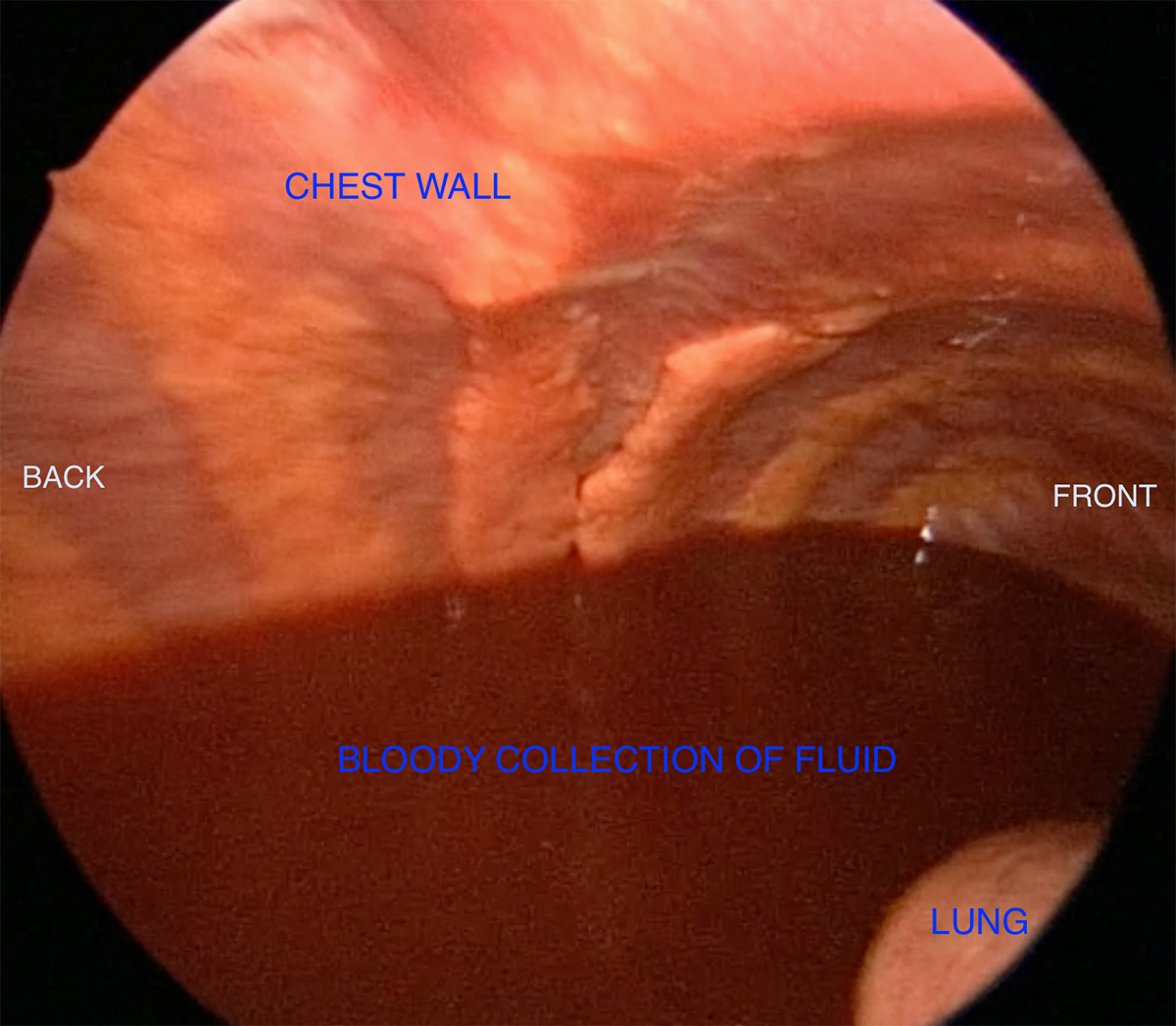
An internal keyhole image (looking up and toward the back of the chest) demonstrating a collection of blood (haemothorax) prior to rib fixation, the blood was drained.
The rib injury is assessed internally as its often easier to see actually where the ribs are broken and how badly they are broken, and the exact location is marked prior to performing a small incision over the broken ribs.
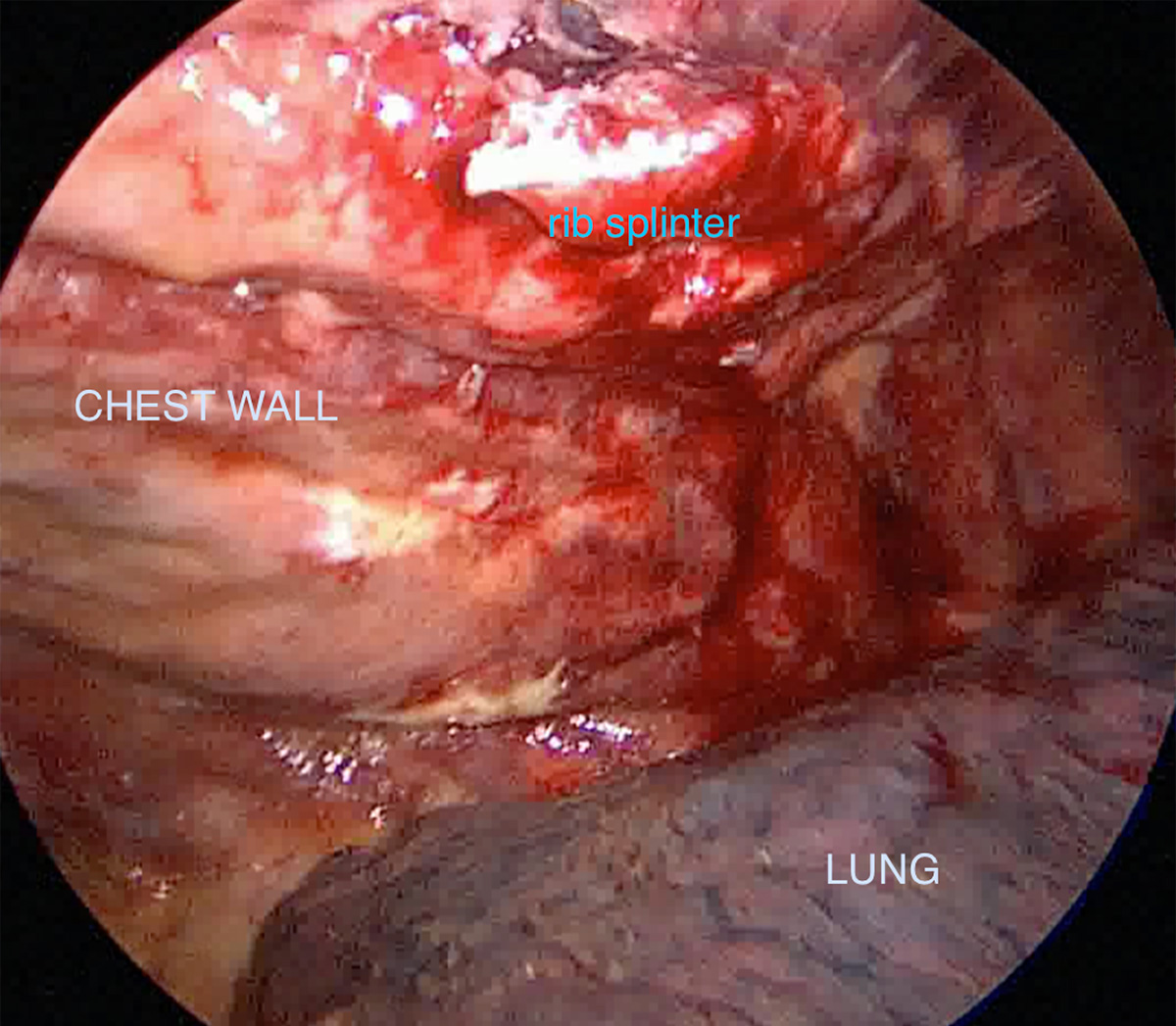
Assessment of rib injury infernally using a keyhole approach showing a rib fracture with a sharp splinter of rib in chest cavity.
A pain catheter (paravertebral catheter) is also inserted under direct vision and to maximise its benefit in relation to which ribs are broken.
Once the incision is made over the broken ribs, the ribs are then exposed, reduced (brought back together) and plated using specialised titanium rib plates and screws locked into the rib on either site of the fracture. A drain is left in the chest cavity and the wound is closed.
Warning: contains images of surgery. Intraoperative Video of Open Reduction Internal Fixation following rib plating
Patients return to the ward, with painkillers and the pain catheter. The drain is removed the next day and most patients go home after 3 days with the help of early mobilisation and physiotherapist. Most patients depending on the age, severity of injury and general health take around 4 weeks to recover from surgery with some restrictions in physical activity.
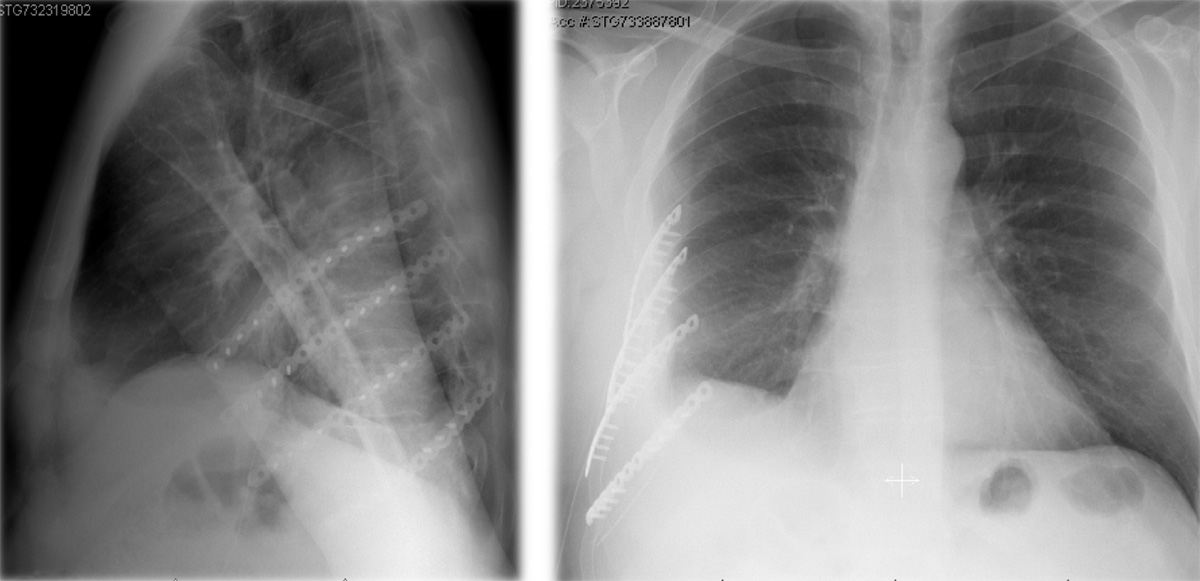
Chest X-ray from the side and front showing multiple rib plates following Open Reduction Internal Fixation after a significant rib injury.
For Sternal injuries, following a general anaesthetic (asleep) an incision is made over the sternal fracture and the fracture reduced (brought back together). The reduced sternum is this held in place using specialised titanium plates and screws locked into the sternum on either site of the fracture.
Sternal fractures through the body of the sternum (red rings) with displacement and deformity (left) following motorcycle accident and with minimal displacement (right) in elderly patient after a simple fall.

Sternal x-ray following open reduction & internal fixation (blue ring)
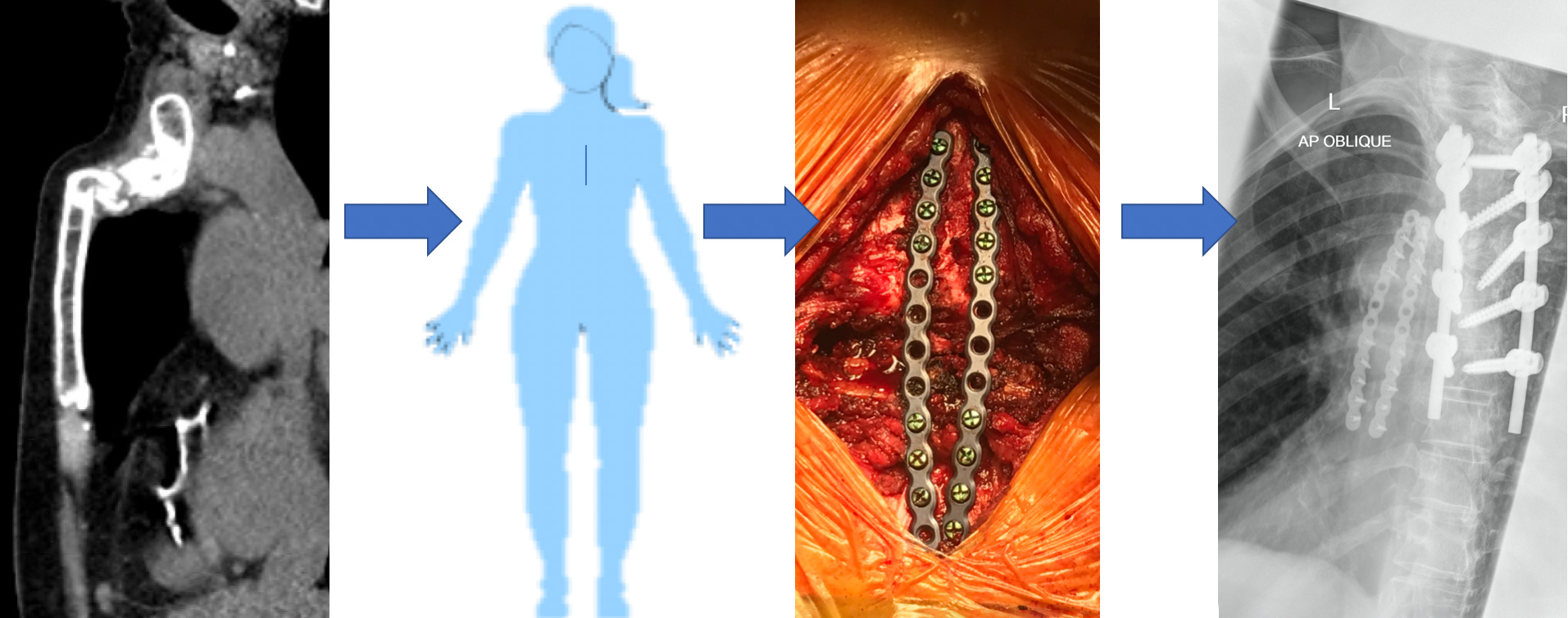
From left to right, A CT scan image of a ‘comminuted’ (fragmented or multiple) sternal fracture, Intraoperative image of reduction and plating and X-ray of plates in position. Note the spinal fixation in the X-ray on the right performed prior to the sternal stabilisation.
Local anaesthetic (LA) is infiltrated into wound and the wound closed usually without the need for a drain. Patients return to the ward, with painkillers. Most patients go home after 2 days with the help of early mobilisation and physiotherapist. Most patients depending on the age, severity of injury and general health take around 6 weeks to recover from surgery with some restrictions on activity particularly heavy lifting.
For complex chest wall injuries, depending on the type of injury Open Reduction Internal Fixation may be an appropriate surgical approach. It is commonly used in Manubriosternal or Costal arch injuries, sometimes used in Costosternal or Costochrondral fracture-dislocations and rarely required for Xiphersternal injuries.
Following a general anaesthetic (asleep) an incision is made over the site of injury and the fracture and/or dislocation reduced (brought back together). The reduced fracture or fracture-dislocation is held in place using specialised titanium plates and screws locked into the bone on either site of the fracture.

X-ray showing costal arch fracture from side
X-ray showing metal plates holding fractured costal arch following internal fixation

Side view of fracture site before (left) and after (right) open reduction internal fixation (red rings)
Local anaesthetic (LA) is infiltrated into wound and the wound closed usually without the need for a drain. Patients return to the ward, with painkillers. Most patients go home after 1-2 days with the help of early mobilisation and physiotherapist. Most patients depending on the age, severity of injury and general health take around 4 weeks to recover from surgery with some restrictions on activity particularly twisting and heavy lifting.
Excision of abnormal area or site of injury
A surgical approach offered occasionally for Rib and sternal injuries and often used for more complex chest wall injuries, as well as surgical treatment of Slipped Rib Syndrome. Excision of the abnormal area or site of injury or fracture site was first described decades ago and its principles remain essentially unchanged, to prevent abnormal movement and friction leading to pain and inflammation, the area or ends of bone/cartilage are excised and separated. In addition to managing chest wall injury, chest wall lumps may also need to be excised. See chest wall lumps.
For Rib Injuries, typically more chronic rib injuries associated with the symptoms of non-union (failure of bone healing), delayed union (still not healing after 6 months) and malunion (doesn’t heal properly). This tends to lead to chronic chest wall pain and tenderness and may be associated with rib fracture displacement which can lead to other problems such as breathing issues or issues of pain and discomfort with certain movements or activities. Excising the site of injury is often effective.
Following a general anaesthetic, an incision is made over the fracture site and the rib or ribs are exposed. If chronic, some healing of the rib ends would have happened (callus formation) and this needs to be excised. The rib ends are then separated creating a small gap, and the wound is closed after Local anaesthetic (LA) is infiltrated, with or without a soft tissue drain left in the wound. The Patient is returned to the ward, with painkillers. Most patients go home after 1-2 days with the help of early mobilisation and physiotherapist. Most patients depending on the age, severity of injury and general health take around 4 weeks to recover from surgery with some restrictions on activity particularly twisting and heavy lifting. By creating a gap between the bone ends, the pain and tenderness caused by malunion or delayed union settles. Non-union can also be treated this way, but if displacement is significant and possibly the source of pain, reduction and internal fixation may be a better option. The small gap typically becomes scarred and though there may be slight movement at the site it prevents fracture ends rubbing and or causing inflammation but generally does not lead to instability.
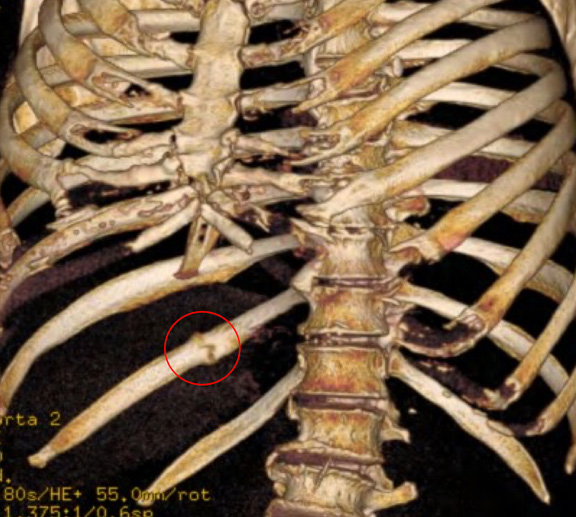
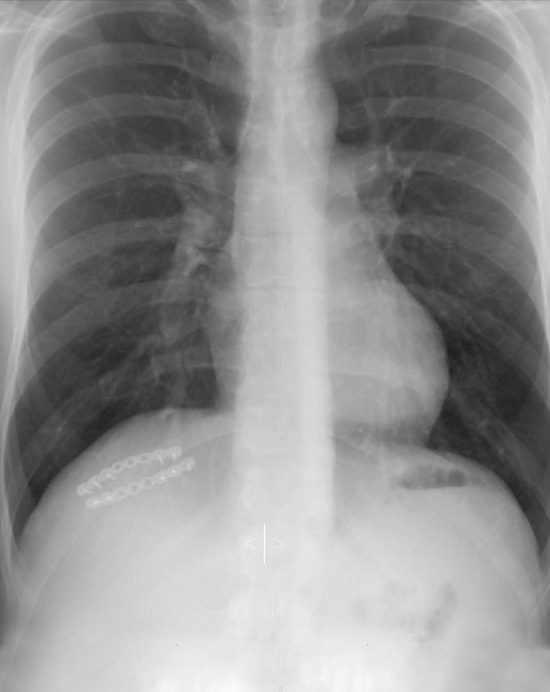
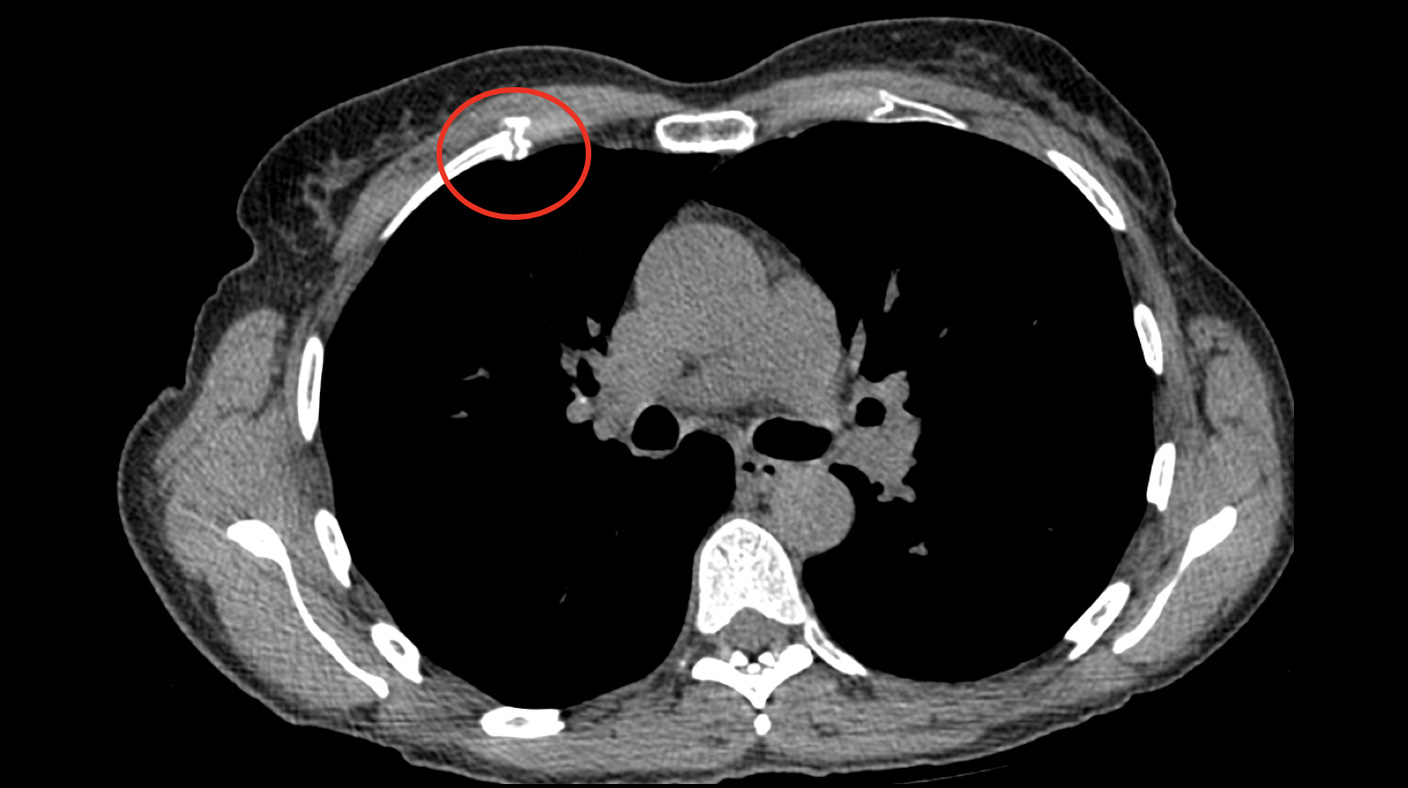
Bone growth around a previous nondisplaced rib fracture (red ring) causing pain and tenderness. Excision without reconstruction resolved pain and discomfort
For Sternal injuries, reduction and internal fixation for stability is the usual choice of operation though if the sternum fracture has become infected, excision of the abnormal area and debridement (removing infected or dead tissue) may be an option.
For Complex chest wall injuries, this approach has advantages as by removing the bone and cartilage ends of the sternocostal or costochrondal fracture-dislocation it removes the source or pain and tenderness without the need for chest wall stabilisation. Internal fixation across the joint of a sternocostal or costochrondal cartilage can be difficult due the placement of plates and screws into potentially soft cartilage on one side of the fracture. which may not ‘support’ the screws leading to failure of internal fixation.
Excision of 5th Sternocostal joint resolved persistent pain and tenderness. The joint was abnormal with evidence of an old fracture dislocation
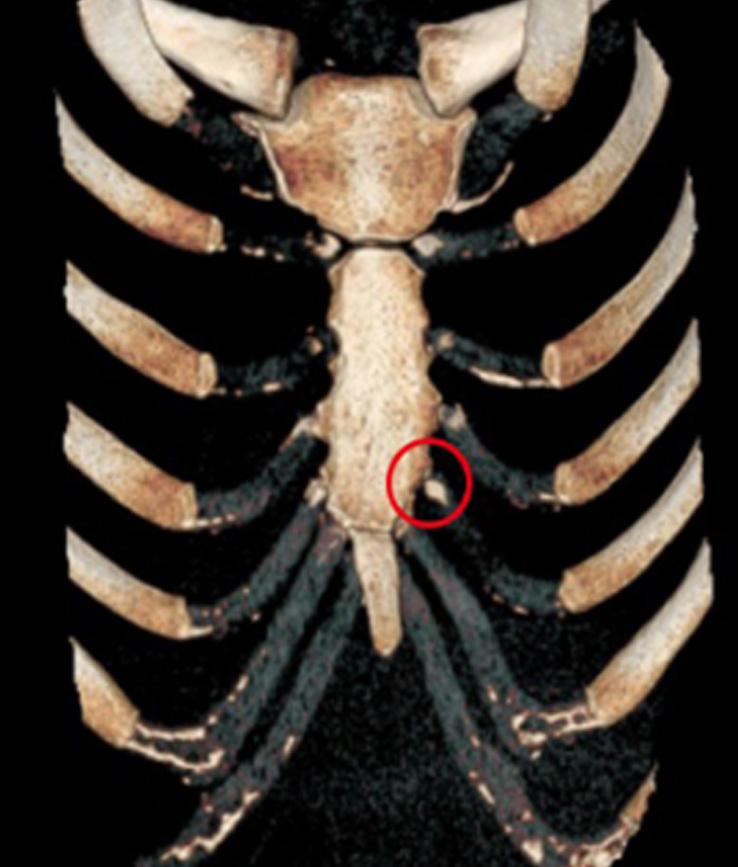
Costochondral fracture with non-union (red ring) with significant pain and tenderness on twisting. Excision of fracture site resolved pain
Surgery of the chest wall may be required to remove an abnormal lump or mass. This may be secondary to a recent trauma, such as evacuation of haematoma (blood in the soft tissues), excision of a benign (non-cancerous) lump or even a chest wall cancerous tumour. These operations are typically performed under a general anaesthetic and involves making an incision over the lump and removing the lump. Local anaesthetic (LA) is infiltrated into wound and the wound closed. A small drain may be left in the wound. Patients return to the ward, with painkillers. Most patients go home after 1-2 days. Most patients depending on the age, severity of injury and general health take around 2-4 weeks to recover from surgery with some restrictions on activity particularly around heavy lifting.
An unusual example of a chest wall problem requiring excision is Elastofibroma Dorsi, a benign pseudo tumour (non-cancerous) that develops around the bottom of the shoulder blade (scapula). It presents with swelling and occasionally pain. Often the presence of swelling and discomfort makes patients prefer surgical excision of the pseudo tumour.
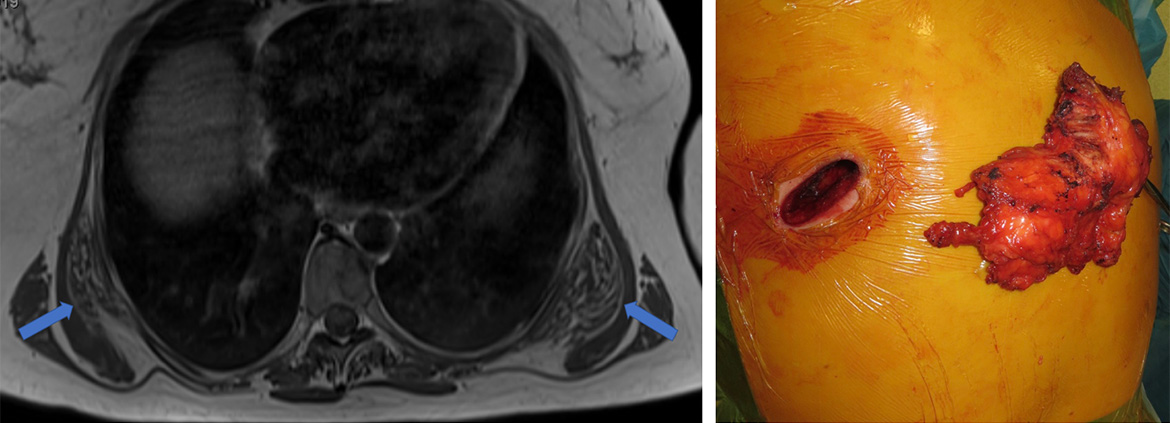
MRI image (left) showing bilateral elastofibroma dors (blue arrows) and following excision of the left pseudo tumour (right). Both tumours were removed.
For Slipped Rib Syndrome, once the excessive movement of a rib tip is diagnosed (typically on ultrasound) as the source of the pain and tenderness, the rib tip can be excised. This is performed under general anaesthetic and involves making a small cut over the area of tenderness at the costal arch. The excessively mobile rib tip is identified and delivered from under the costal arch and then excised preventing the rib tip from ‘sliding’ under the costal arch. Typically, it involves the floating ribs 8, 9 and 10 and occasionally can be more than one rib tip.
Local anaesthetic (LA) is infiltrated into wound and the wound closed usually without the need for a drain. Patients return to the ward, with painkillers. Most patients go home after 1 day. Most patients depending on the age, severity of injury and general health take around 4 weeks to recover from surgery with some restrictions on activity particularly twisting and heavy lifting.

The rib associated with excessive is identified on pre-operative ultrasound and intra-operatively. In this case it is the left 9th rib tip. It is grasped (Left), delivered from under the costal arch (middle) and excised (right).
Repair and reconstruction of chest wall
In more complex cases of chest wall problems including lung hernia (lung coming between ribs) following Rib injury, repairs of diaphragm or excision of Chest wall lumps particularly if cancerous, combinations of approaches including excision of the abnormal area, with Open reduction and internal fixation of bony structures and finally reconstruction of the chest wall may be required.
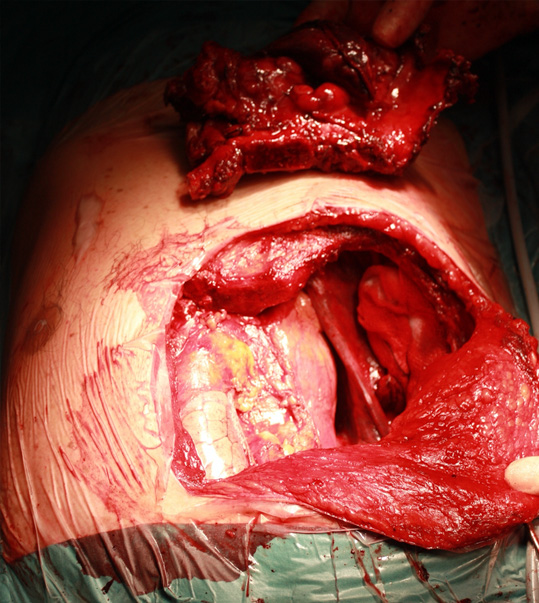
Warning: contains images of surgery
The intraoperative images show removal of a malignant tumour involving the sternum and several ribs and the subsequent repair and reconstruction of the chest wall (from left to right).
 Beginning of operation to remove a tumour of the sternum
Beginning of operation to remove a tumour of the sternum
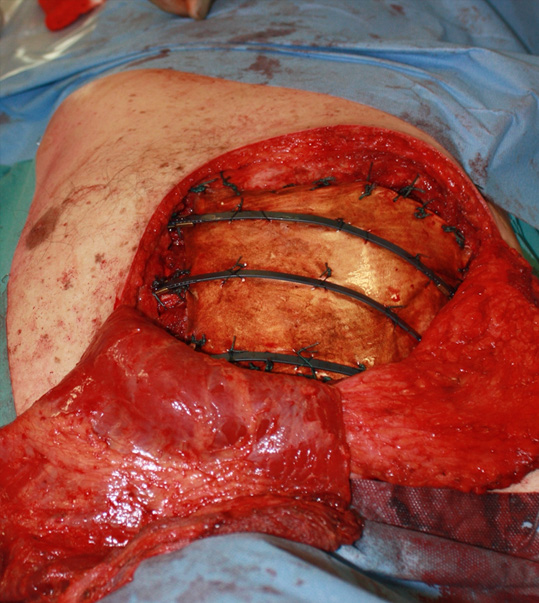
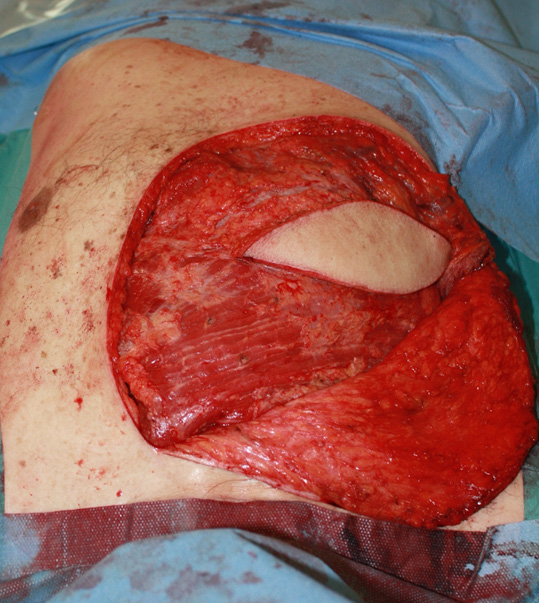
 At End after excision of tumour and reconstruction of the chest
At End after excision of tumour and reconstruction of the chest
An unusual example of Repair and reconstruction of the chest wall is an operation called a modified Ravitch performed for a developmental abnormality of the chest wall called pectus carinatum.
Modified Ravitch Procedure – pectusclinic.com Find out more

Radiology Image on left shows protruding chest and to the right following correction using metal plates to reconstruct the sternum and chest wall and correct pectus carinatum