Chest wall lumps
Chest wall injuries, inflammatory or infective conditions and even cancerous or non-cancerous growths can lead to the development of a chest wall lump. The chest wall is made up of bone (sternum, ribs and thoracic spine), cartilage and other ‘soft tissues’ including muscles, tendons, ligaments, fascia (membranes), blood vessels, nerves, lymph vessels and nodes. Any of these can lead to the development of a chest wall lump. In addition, underlying organs such as the lung, the lining of the lung (the pleura) or conditions in the cavity of the chest (the pleural cavity) can also lead to chest wall lumps. NOTE: The Rib Injury Clinic does NOT treat Breast Lumps.
The chest wall can be divided into three layers:
- Superficial layer: Skin and subcutaneous fat
- Intermediate layer: Shoulder girdle and pectoralis muscles
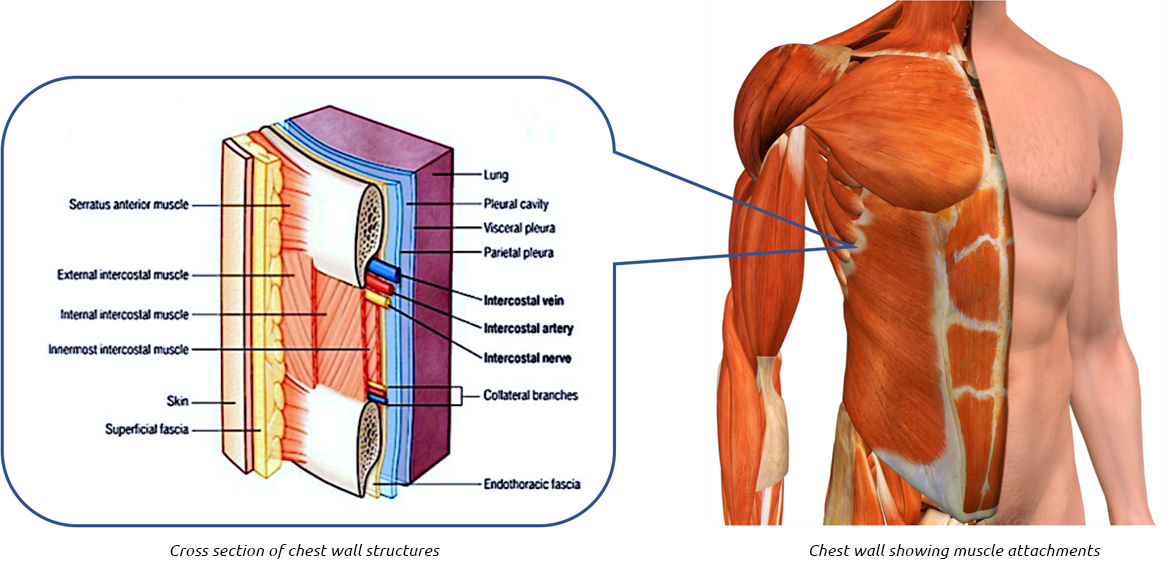
- Deep layer: Bony chest including sternum, ribs, thoracic spine and Pleural lining including the intercostal space, fascia, and pleural
Chest wall lumps can come from any of these layers and their components including the blood vessels and nerves that course through them.
Symptoms
Depends on what the chest wall lump is caused by, but along with the lump or deformity there may be associated pain, swelling, inflammation (redness), discharge, clicking or altered sensation. If large they can cause a restriction of certain movements. The lump may develop quickly such as an abscess, or slowly or become noticeable with significant weight loss or with certain activities for example a lung hernia.
Congenital and Developmental Abnormalities
Chest wall asymmetry (variation between one side and another) is common and often presents in childhood as a lump in the anterior chest wall. It may be related to scoliosis (curvature of the spine) presenting with a lump on the chest on the opposite side to the curvature along with uneven shoulders and/or hips. Pectus deformities - pectus excavatum and particularly pectus carinatum can present with a ‘lump’ in the anterior chest wall.


Pectus carinatum in a 14 year old boy. It developed during a rapid growth spurt over a year
Pectus Carinatum Bracing treatment – pectusclinic.com Find out more
Pectus deformities can be present at birth or within the first year, but often only become noticeable during puberty. Associated musculoskeletal abnormalities such as Marfan syndrome, Ehlers-Danlos and Poland Syndrome are common but other associated conditions include Congenital heart disease, osteogenesis imperfecta, muscular dystrophy, Pierre Robin Syndrome, Turner Syndrome, and prune belly Syndrome.
Rib Abnormalities and anatomical variations of ribs can cause an ‘apparent’ chest wall lump. One of the more common variants is Prominent Convexity of the anterior rib/s presenting at a young age. It’s important to differentiate this from a pectus carinatum deformity.
Other types of rib abnormalities presenting with an apparent chest wall lump include rib Segmentation and Fusion Anomalies leading to abnormally shaped ribs for example bifid rib, fusion or bridging between ribs or smaller (hypoplastic) or missing ribs (absent) as in Poland’s Syndrome.
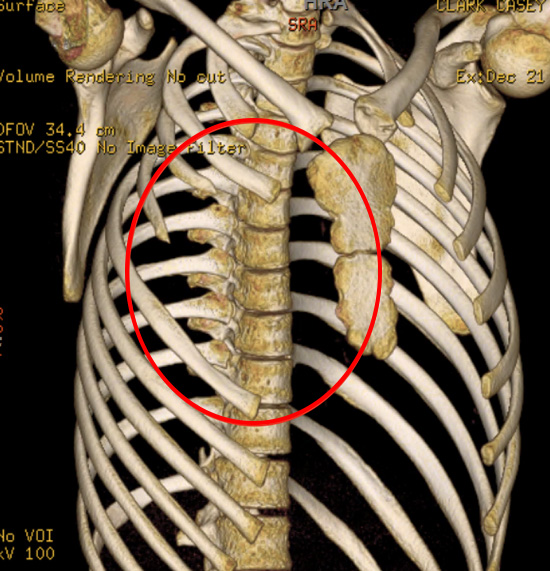
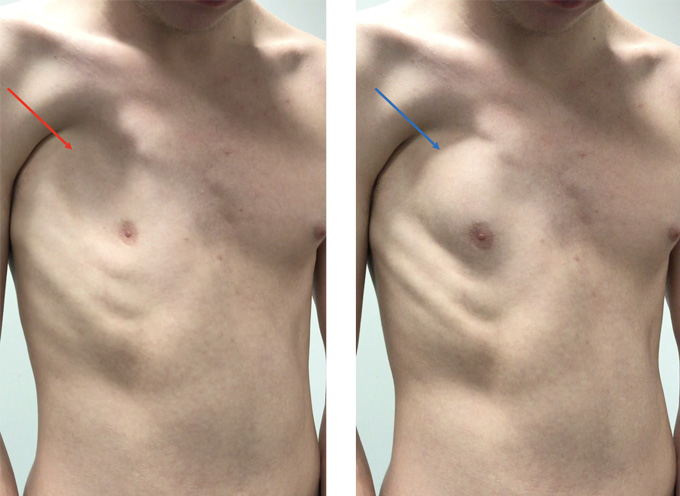
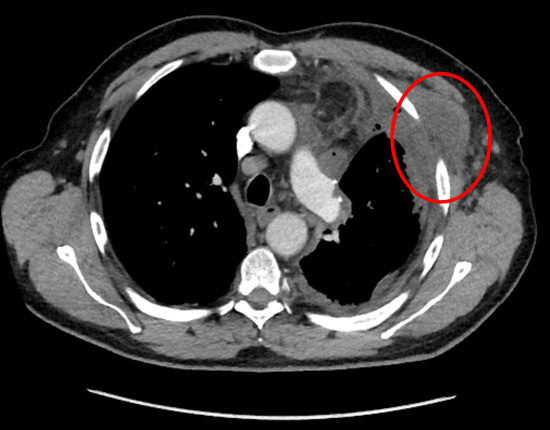
Young man with Poland’s syndrome. Note missing right pectoralis muscle and upper ribs at front (red ring). When he breathes in, due to missing upper anterior ribs, chest wall draws inwards (left image, red arrow) and then when he breathes out, lung bulges outwards (right image, blue arrow)
Supernumerary or extra ribs can also be seen, the most common is cervical ribs, arising from the 7th cervical vertebrae, on one or both sides. It does not present with a chest wall lump but can cause temporary loss of feeling, weakness or tingling in the affected arm and fingers.
Benign Chest Wall lumps
Various benign (non-cancerous) conditions or growths can cause a chest wall lump to develop. They can be divided into benign soft tissue tumours and bony benign tumours of the chest wall.
Benign tumours of the chest wall
| Soft tissue (skin, fat and connective tissue) | Bony (Skeletal) |
|---|---|
| Lipoma | Fibrous dysplasia |
| Fibroma (eg dermatofibroma, elastofibroma dorsi) | Aneurysmal bone cyst |
| Schwannoma | Giant cell tumour |
| Neurofibroma | Chondromyxoid fibromas |
| Ganglioneuroma | Ossifying Fibromyxoid tumour |
| Paraganglioma | Osteochondroma |
| Haemangioma | Osteoid osteoma |
| Lymphangioma | Enchondromas |
| Solitary fibrous tumour |
Benign Soft tissue tumours
Lipoma is a benign tumour made of fat tissue. They can be occasionally multiple and are generally soft painless and movable to the touch. They usually occur just under the skin, but occasionally may be deeper. Most are less than 5 cm in size. They can occur on the chest and upper back.
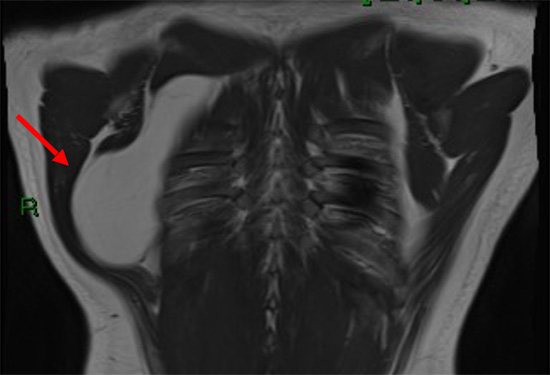
Large Lipoma (red arrow) involving the intermediate chest wall structures and affecting shoulder movements
Fibromas are another type of benign tumours that are composed of fibrous or connective tissue. They can grow in all organs, arising from mesenchyme tissue including the chest wall. They can be described as hard fibromas; in the skin this is called dermatofibroma (a fibrous nodule of the skin). Keloid scars are a type of hard fibroma. Or soft fibromas or skin tags. There are other types of fibroma depending on their origin, composition and location. Elastofibroma dorsi is a benign soft-tissue tumour with a characteristic location and imaging appearance.
Peripheral Nerve Tumours are growths originating from nerves or the nerve coverings. They can occur anywhere in the body including the chest wall. Schwannomas, also known as neurilemomas or neurinomas, are benign tumours that originate in nerve sheaths and are usually slow growing. Chest wall schwannomas arise from spinal nerve roots and intercostal nerves and typically occur in patients between 20 and 50 years of age. Neurofibromas are slow-growing neoplasms that originate from a nerve, may or may not be encapsulated, and may include components of cystic degeneration and calcification. Neurofibromas develop most commonly in patients between the ages of 20 and 30 years. Along with Ganglioneuroma and Paraganglioma, peripheral nerve tumours tend to be picked up incidental on x-ray or occasionally are associated with altered sensation or pain but rarely cause a chest wall lump as they tend to grow in the chest cavity.
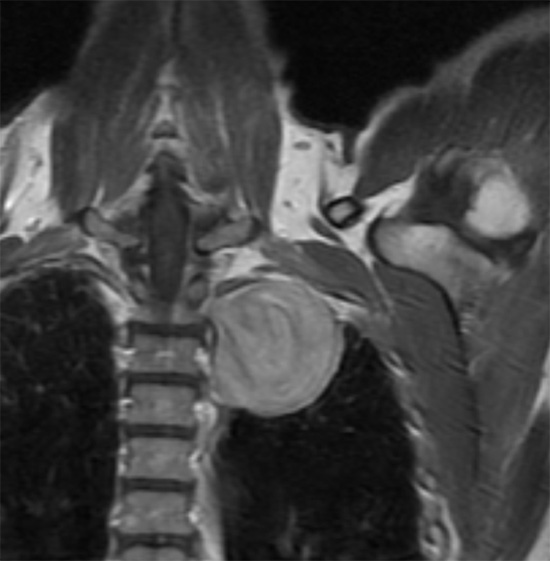
MRI Image of a large Schwannoma in the left upper chest cavity a middle-aged man with left arm and shoulder pain but no no chest wall lump. It was removed surgically
Vascular Chest wall Tumours refer to growths arising from blood vessels and include Cavernous haemangiomas, typically superficial growths consisting of dilated, tortuous, thin-walled vessels. Similar to vascular chest wall tumour, lymphangiomas are benign tumours caused by lymphatic malformations. When superficial they are soft, non-tender masses with a doughy consistency. Cystic lymphangioma of the chest wall is rare.
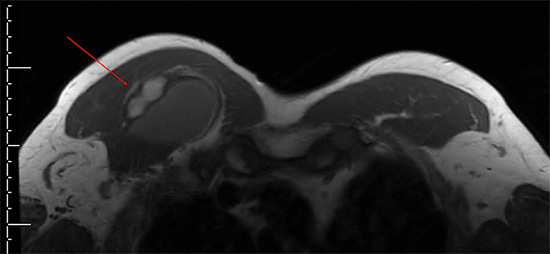
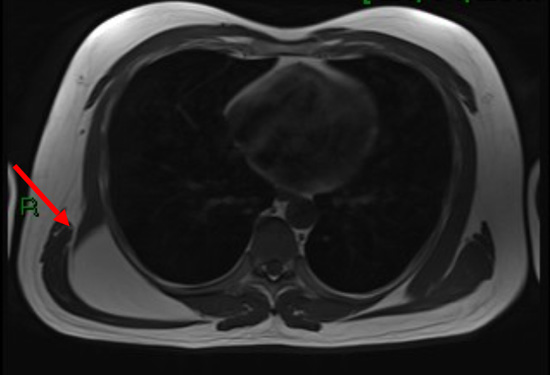
MRI image of a right swollen pectoralis muscle with an underlying lymphangioma (red arrow). It was surgically removed
Solitary fibrous tumours are rare growths of soft tissue cells that can form nearly anywhere in the body. They most commonly occur in the lining of chest wall (the inner or pleural lining). Most are benign though they can become malignant. They very rarely cause a chest wall lump.
Benign Bony tumours
Fibrous dysplasia is an uncommon bone disorder in which scar-like (fibrous) tissue develops in place of normal bone. This irregular tissue can weaken the affected bone and cause it to deform or fracture. It can affect the ribs and rarely the sternum. It tends to affect a single rib (monostotic) and more severely multiple bones (Polyostotic). The majority of monostotic lesions have no symptoms and its discovered incidentally on x-ray. Symptomatic patients can have pain, possibly secondary to a pathologic fracture, or with an obvious deformity.
An aneurysmal bone cyst is a benign, but expansile tumour like lesion that generally occurs in the long bones including the vertebral column and rarely in the chest wall. A giant cell tumour is a rare, aggressive non-cancerous tumour. It usually develops near a joint at the end of the bone. Most occur in the long bones of the legs and arms. Giant cell tumours most often occur in young adults when skeletal bone growth is complete. It is very rare in the ribs and chest wall. Other types of benign bony tumours that can occasionally affect the chest wall causing a chest wall lump or chest wall symptoms include Chondromyxoid fibromas are a type benign cartilaginous tumours which occasionally occur in the ribs, spine, or scapulae and rarely the sternum; Ossifying Fibromyxoid tumour which rarely affects the chest wall but can lead to a slowly growing painless mass and Enchondromas, a more common benign cartilage tumour found inside bones including rib bones.
An exostosis, also called a bony spur, occurs when a bony growth extends beyond a bone's usual smooth surface. Exostosis can cause chronic pain or irritation, depending on its size and location. See chest wall pain. Sometimes, cartilage will grow over an area of exostosis, which is called osteochondroma. These are a common benign bony tumour but a rare tumour in the ribs and chest wall.
Malignant chest wall tumours
The most common malignant tumours affecting the chest wall are called metastasis, cancers that arose elsewhere, such as the lung, colon or breast and have spread to either the soft tissues or especially the bony skeletal of the chest wall. Bony metastasis can lead to pain and deformity as well as risk of rib or even sternal fracture (pathological fracture).

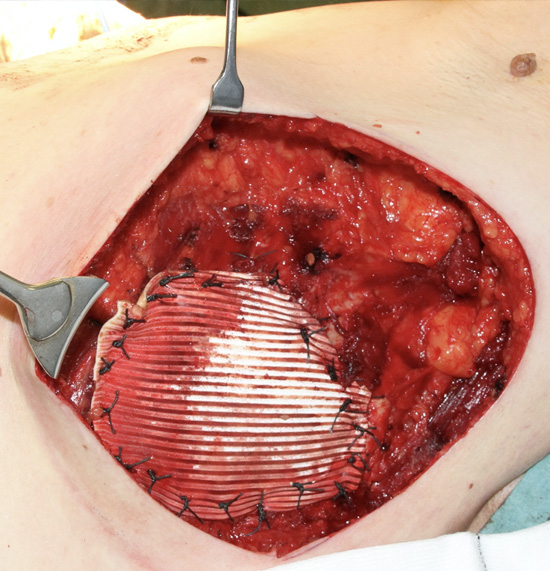
A locally invasive breast cancer that has spread into chest wall that was removed ‘en-bloc’ (all together) with the left breast and part of the chest wall and then reconstructed
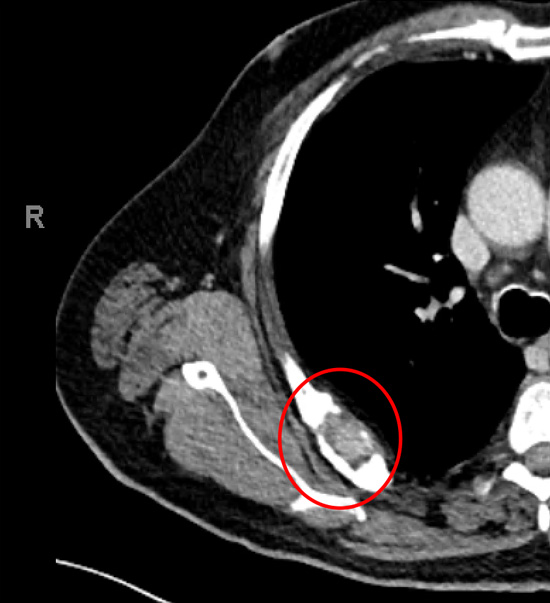
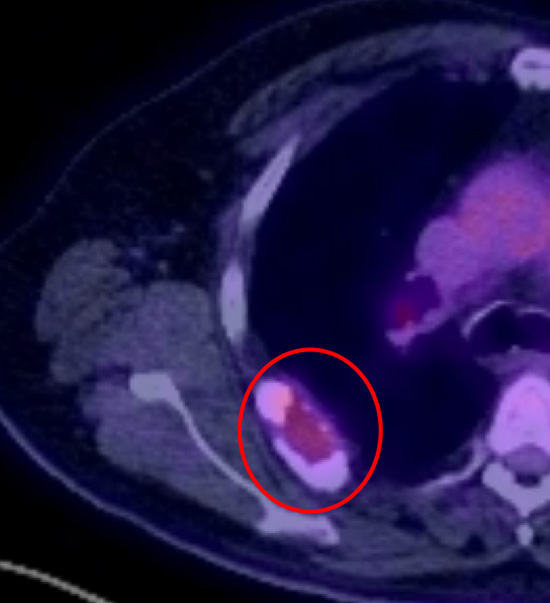
Secondary (metastasis) cancer to the 7th right rib causing pain on moving the shoulder (red rings) on chest CT (left) and PET (right). The original cancer was from the thyroid. The rib and cancer were surgically removed
Malignant tumours of the chest wall
| Soft tissue (skin, fat and connective tissue) | Bony (Skeletal) |
|---|---|
| Rhabdomyosarcoma | Secondary cancers (metastasis) |
| Ewing sarcoma | Myeloma |
| Leiomyoscarcoma | Chondrosarcoma |
| Angsiosarcoma | Osteosarcoma |
| Neuroblastoma | |
| Ganglioneuroblastoma | |
| Malignant fibrous Histiocytoma | |
| Malignant Peripheral nerve sheath tumour | |
| Malignant Solitary fibrous tumour | |
| Dermatofibrosarcoma |
Most of these malignant soft tissue and bony tumours can affect any part of the body including the chest wall though most are rare in this part of the body. They form a group of cancers called Sarcomas, a broad group of cancers that arise from connective tissue cells that include bone, cartilage, fat, muscle and blood vessels.
Malignant Soft tissue tumours
Sarcomas include Rhabdomyosarcoma, is an aggressive and highly malignant form of cancer that develops from skeletal muscle cells anywhere in the body. It is generally considered to be a cancer of childhood. Ewing's sarcoma is a type of cancer that forms in bone or soft tissue. Symptoms may include swelling and pain at the site of the tumour, fever, and a bone fracture. The most common areas where it begins are the legs, pelvis, and chest wall. Leiomyosarcoma is a rare type of cancer that affects smooth muscle tissue. These tumours are most common in the abdomen but can occur anywhere in the body. Angiosarcoma is a rare type of cancer that forms in the lining of the blood vessels and lymph vessels.
Neuroblastoma is a rare type of cancer that mostly affects babies and young children. It develops from specialised nerve cells (neuroblasts) left behind from a baby's development in the womb. It occurs in the adrenal glands situated above the kidneys, or in the nerve tissue that runs alongside the spinal cord in the neck, chest, tummy or pelvis. Ganglioneuroblastoma is a tumour that also arises from nerve tissues and is regarded as an intermediate tumour, one that is between benign (slow-growing and unlikely to spread) and malignant (fast-growing, aggressive, and likely to spread). Both Malignant Peripheral nerve sheath tumour and Malignant Solitary fibrous tumour arise from the same cells as the benign counterparts but behaviour more aggressively, with local and/or distant spread. Dermatofibrosarcoma is a rare type of cancer, a soft tissue sarcoma that develops in the deep layers of skin. It is sometimes described as having tentacles that can grow into surrounding fat, muscle and even bone. It can present on the torso.
Malignant Bony tumours
Myeloma is a type of cancer that develops from cells in the bone marrow called plasma cells. Bone marrow is the spongy tissue found inside the inner part of some of our large bones. The bone marrow produces different types of blood cells. It often presents in older patients with bone pain often in the back or ribs though a chest wall lump is unusual. Related to myeloma, Solitary bone plasmacytomas is an uncommon plasma cell tumour which is localized to bone. They may involve any bone, but they have a predisposition for the red marrow-containing axial skeleton including ribs and sternum.
Examples of bony sarcomas, Chondrosarcoma is a cancer composed of cells derived from transformed cells that produce cartilage whereas An Osteosarcoma (OS) or Osteogenic sarcoma (OGS) (or simply bone cancer) is a cancerous tumour in a bone.
Infectious causes of chest wall lumps
Infections of the chest wall can often lead to inflammation and pain in the affected area. They are usually caused by bacteria, occasionally viral illness and rarely fungal infection. The infection may arise from the chest wall itself, for example from a skin infection leading to a chest wall abscess. Alternatively, the chest wall infection may come from the inside and be caused by a pneumonia (chest infection) that spreads to the pleural cavity (para-pneumonic effusion) which itself becomes infected (an empyema). Rarely, infection comes from another site such as the underlying bone, such as the ribs or sternum. Bone infection is known as Osteomyelitis.
Symptoms
The most common symptoms are chest wall swelling with localised pain and tenderness, typically persistent, worse on breathing deeply or with certain activities. The pain and swelling may be associated with a fever, ‘flu-like illness’ and chest symptoms such as a cough. Diagnosis is usually clinical along with blood tests and X-rays.
Types of chest wall infections include:
- Pleurisy — infection or inflammation of the thin membranes (pleura) of the chest wall leading to chest wall pain particularly when breathing in. It may be associated with pleural effusion (collection of fluid) in the chest cavity.
- Empyema necessitans – Following a pneumonia If the associated fluid (para-pneumonic effusion) in the chest cavity becomes infected it can lead to a empyema (infection of the pleural or chest cavity). Empyema necessitans refers specifically to extension of the empyema into the neighbouring chest wall.
- Chest wall Abscess – Appears as a hot, swollen and tender lump which can sometimes be associated with overlying skin redness (cellulitis). It can even discharge (burst).
- Osteomyelitis – Bone infection classically of the upper sternum and the sterno-clavicular joints can lead to swelling and pain. It is a rare of chest wall infection.
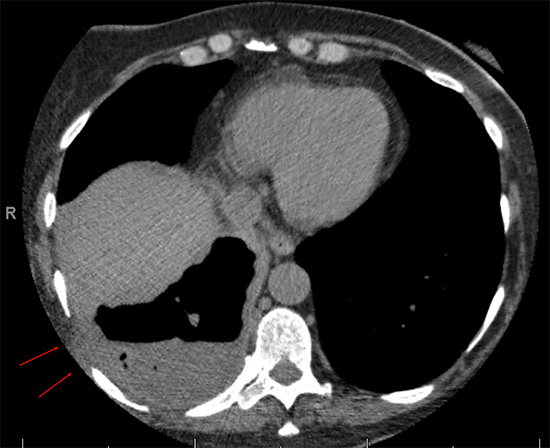
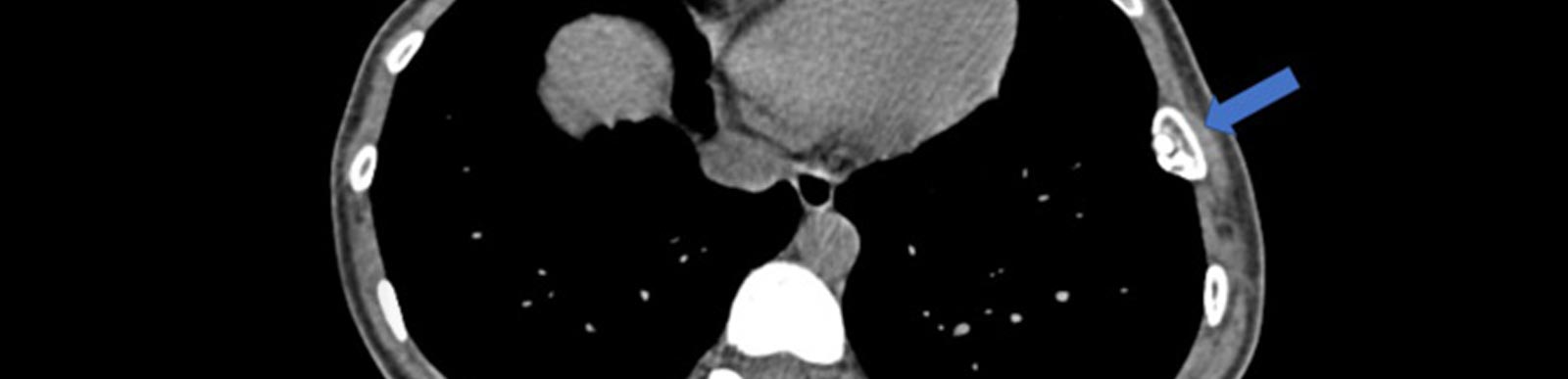
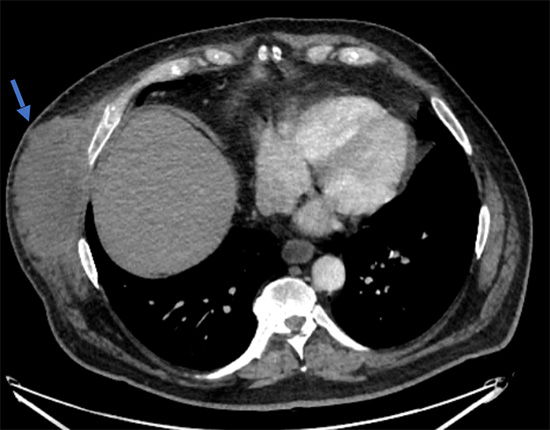
Empyema necessitans: Chest CT scan of an elderly lady with underlying health issues with a right sided empyema that is starting to extend into the chest wall (red arrows)
Chest wall infections may be associated with certain types of infection, such as Tuberculosis or be secondary to recent chest or heart surgery or following chest trauma.

Chest CT scan of a chest wall abscess (blue arrows) in middle aged overweight diabetic man. The abscess required an operation called an incision and drainage
Traumatic causes of chest wall lumps
Following chest wall trauma, either immediately, shortly after or many months following the injury a chest wall lump can develop depending on the cause.
Immediately or within a few hours following a chest injury, the chest wall can become bruised and begin to swell. A chest wall Haematoma is caused by a build-up of blood in the soft tissues of the chest wall (superficial) but can be deeper (intermediate) or in the chest cavity itself (deep). This is called a Haemothorax (blood in the chest cavity). The severity and seriousness of a haematoma depends on whether there is still active bleeding, as well as the size and location.
Chest Wall haematoma (red ring) following a surgical procedure.
Rib or sternal fractures if badly displaced can lead to a chest wall lump that may become painful and tender and lead to deformity and a restriction of activities. See Rib and Sternal injuries. Following the original fracture, the bone ends typically begin to heal and lay down bone callus (a connecting bridge a bone fracture made of bone and cartilage cells) followed by remodelling of the bone and healing. If the bone end were badly displaced and/or the patient has impaired healing, the bone (typically the rib but occasionally the sternum) may fail to heal properly. See complications of rib injury.
Following a chest wall injury, due to degeneration or a chronic inflammatory condition such as Osteoarthritis, bony projections (exostosis) or bony spurs (Osteophytes) can develop along bone edges particularly joints and the spine. They are unusual in the skeletal chest wall and rarely cause symptoms but can cause persistent pain and tenderness particularly on certain movements such as twisting. See chest wall pain.
Treatment
Chest wall lumps once diagnosed can be treated either conservatively involving reassurance, rest, restrictions of activities and painkillers, or through some form of intervention including targeted physical therapy, drainage or a variety of surgical options including excision (removal) depending on what the underlying cause is. See Treatments.