
Chest wall pain
The chest wall is made of bone, cartilage, ligaments and tendons and covered by muscle and soft tissues. The chest wall is designed specifically to protect the organs it surrounds and support respiration.
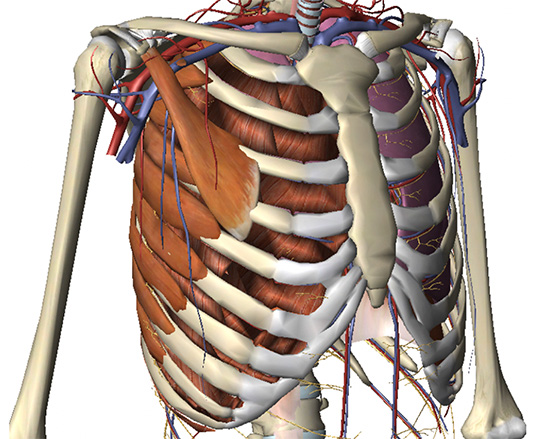
The chest wall showing the bony skeleton, cartilage, muscle attachments & blood supply
With respiration the rib cage is designed to expand and contract with breathing in and out. The ribs and their connections to the sternum at the front and spine at the back act to facilitate that by moving up and down in a particular way, what is described as ‘bucket handle’ and ‘pump handle’ movement.
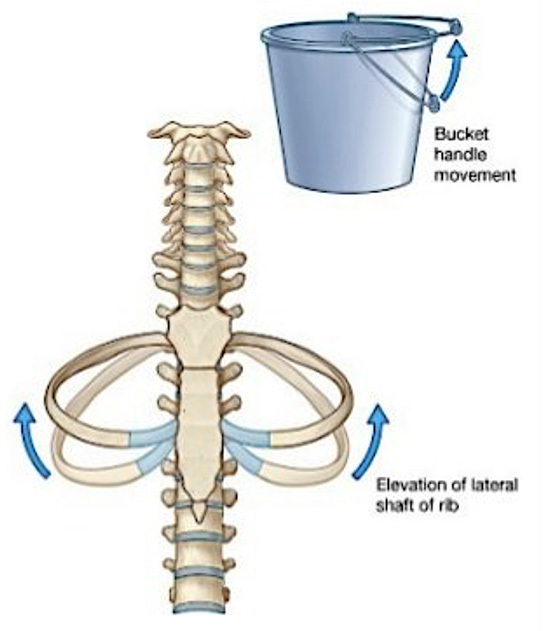
Bucket-handle is a movement of ribs that results in change in transverse diameter of the thorax
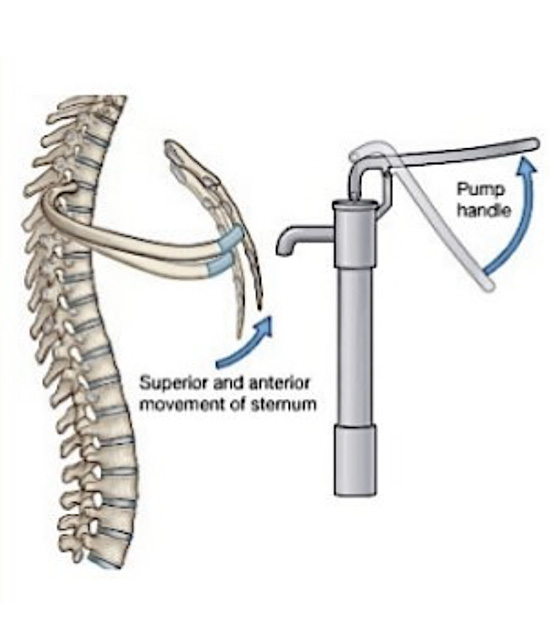
Pump-handle is a movement of the ribs that results in a change in the anteroposterior diameter of the thorax
Movements of the rib cage that support breathing in and out
These movements are made possible by joints of the ribs, particularly the true ribs (vertebrosternal ribs) to the vertebrae (the costovertebral and costotransverse joints) and to a lesser extent at the sternum (the costosternal joints).
Created for the rib injury clinic by AnatomikModeling
3D interactive chest wall model showing rib cage, thoracic spine and sternum with costal cartilage
The costal cartilage are segments of cartilage that connect the sternum to the ribs and help to extend the ribs into a forward motion. This cartilage also contributes to elasticity within the walls of the thorax, allowing the chest to expand during respiration.
The complex nature of thorax with multiple joints and cartilaginous connections coupled with a need to continually move (breath) makes it prone to inflammatory conditions and chronic pain problems.
Symptoms
The most common chest wall symptom is pain. The type of pain and its location depends on the underlying cause of the pain. The pain may be an ache, constant or occasional, sharp, stabbing or burning. The pain may be mild to severe. The pain may worse on certain movements such as deep breathing, coughing or twisting. It may be associated with numbness, tingling or a ‘radiating’ pain, from front to back for example.
The causes of chest wall pain are numerous but are most commonly musculoskeletal conditions, though other conditions often need to be excluded first. The most common cause of chest wall pain is from through some form of direct trauma or injury to chest wall with underlying swelling and inflammation to the soft tissues.
Musculoskeletal causes of isolated chest wall pain
| Most Common | Less Common |
|---|---|
| As a result of direct Injury or trauma to chest | Stress fractures |
| Costochondritis | Tietze’s syndrome |
| Slipped Rib Syndrome or lower rib pain syndromes | Xiphoidalgia |
| Pain radiating from thoracic spine or costovertebral joints | Spontaneous sternoclavicular subluxation |
| Intercostal muscle strain or pulled chest muscle | |
| Sternalis syndrome |
Costochondritis refer to Inflammation of the cartilage junctions of the sternum and ribs typically felt at the costosternal and costochondral joints. It is a relatively common condition seen in adult and patients who develop pain and tenderness at the front of the chest. It’s felt over the affected cartilage segments in multiple areas, usually on one, or occasionally both sides of the sternum. The most common sites of pain are the anterior cartilage segments of the 2th to 5th ribs at the front of the chest near where the ribs join the breastbone. This pain increases with activity, moving or twisting or when taking deep breaths. Conversely, it decreases as movement stops or with quiet breathing. The reproducible tenderness but without swelling you feel when you press on the sternal and rib joints (costosternal and costochondral junctions respectively) is a constant feature of costochondritis. Without this tenderness, a diagnosis of costochondritis is unlikely.
The cause is unknown but may be associated with unusual or excessive physical activity, minor trauma particularly repetitive and/or excessive over of use of arms. Occasionally, it can follow a viral infection or rarely a bacterial or fungal infection in patients prone to such infections.
There also appears to be a relationship between chest wall deformities and costochondritis and certainly younger patients with pectus excavatum and carinatum complain of cheat wall pain though it’s difficult ascertain whether this is costochondritis, idiopathic chest wall pain (chest pain in children without an obvious cause) or chest wall pain caused by the anatomical deformity associated with pectus.
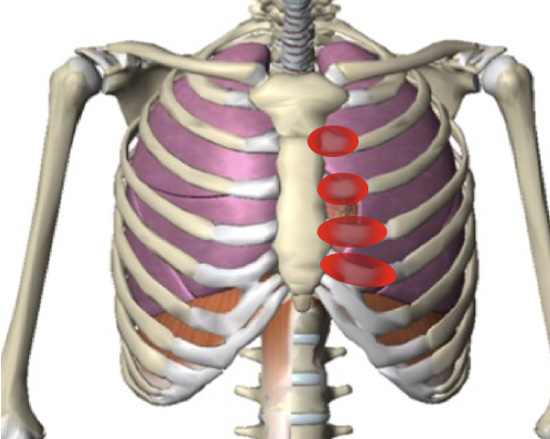
Typical location of pain and tenderness noted in Costochondritis
Tietze syndrome is often confused with costochondritis but is rarer and importantly associated with sudden chest pain and localised swelling at junction of the ribs and breastbone. It usually affects the junctions at the 2nd and 3rd ribs. The swelling may last for several months and often radiates to the arms and shoulders. The cause is unknown.
For Lower rib pain syndromes. See Slipped rib syndrome. Pain originating from the thoracic spine and specifically from the ‘spinal-rib complex’ is common. The pain experienced in the front or side of the chest is described as referred pain and may arise from the posterior thoracic spinal structures including the intervertebral discs and facets. Costotransverse disorders or costovertebral joint dysfunction are disorders affecting or involving specifically the costotransverse and costovertebral joints and ligaments which are felt to be related to pain experienced in the thorax. See other associated problems.
Muscle strain or a ‘pulled muscle’ refers to muscle overstretching leading to a partial or complete tear and can occur in any muscle. Muscles affected tend to be in ones that cross two joints; exposed to sudden explosive action, such as sprinting and the hamstrings; or following periods of overtraining. In the chest, sudden twisting or movement ‘at the torso’ particularly against resistance can lead to an intercostal muscle strain. The diagnosis is a clinical one, that is relying on the clinical history and examination as the muscle and injury to it, is hard to ‘see’ using radiology (MRI and ultrasound) and so grades of muscle strain are hard to allocate to intercostal muscle strain. The pain is typically sharp and stabbing immediately but typically becomes a dull ache overtime and can be associated with swelling, muscle spasms, difficulty moving the affected area, pain while breathing and even bruising.
Muscle strains can be categorized into three grades, based on severity
| Grade | Features |
|---|---|
| Grade 1 | Mild damage to individual muscle fibres (less than 5% of fibres) that causes minimal loss of strength and motion. |
| Grade 2 | More extensive damage with more muscle fibres involved. However, the muscle is not completely ruptured. These injuries present with significant loss of strength and motion. |
| Grade 3 | Complete rupture of a muscle or tendon. These can present with a palpable defect in the muscle or tendon. However, swelling in the area may make this difficult to appreciate. |
Activities and Sports that may cause chest wall muscle strain:
| Intercostal muscle | Pectoralis muscle | Latissimus dorsi | Serratus muscle |
|---|---|---|---|
| Weight training (side to side against resistance) | Weight training (bench press) | Weight training (bench press) | Weight training (heavy weights) |
| Heavy lifting with side bending, twisting or turning | Heavy lifting from front to chest height | Heavy lifting with upper body | Repetitive motions against resistance |
| Bowling | Rugby | Climbing | Swimming |
| Cricket, Baseball (bowling, throwing) | Skiing | Cricket, baseball & throwing activities | Tennis |
| Rowing | Wrestling | Rowing | |
| Tennis | Hockey | Tennis | |
| Hockey | Parachuting |
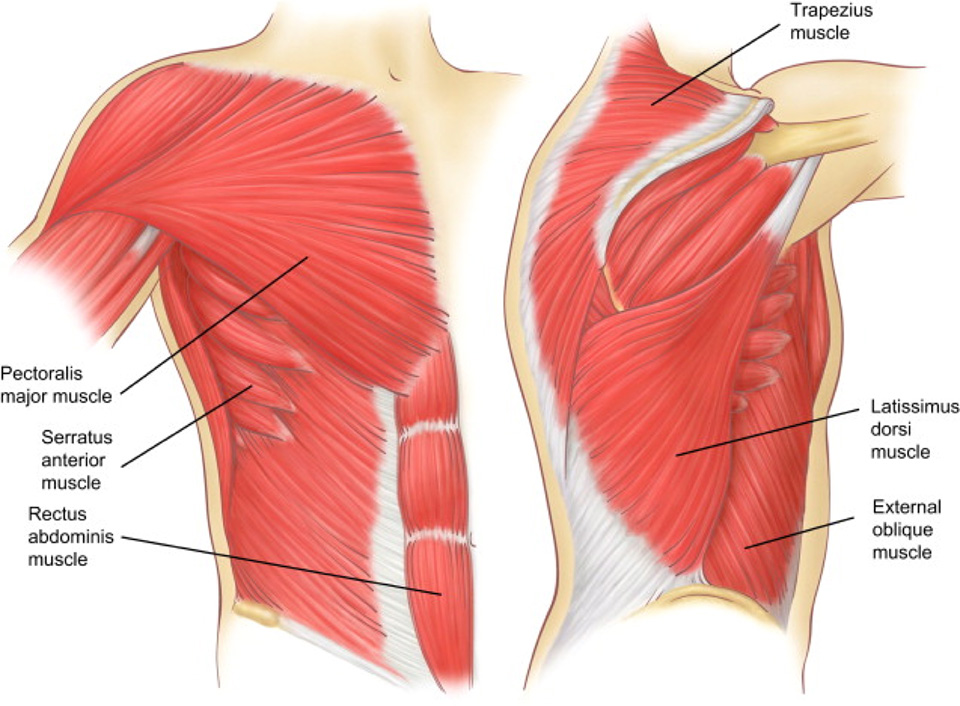
Large chest wall and abdominal muscles
Larger chest wall muscle groups can also be strained. The Pectoralis major muscle is a large muscle at the front of the chest. It used to rotate the arm inwards, pull a horizontal arm across the body, pull the arm from above the head down and pull the arm from the side upwards. Pectoralis Major strain can happen during vigorous sports activity classically weight training. Its weak point is where the pectoralis or pec muscle tendon attaches to the upper humerus (arm bone) though rarely its tendinous insertion to the upper ribs and sternum can also tear. Symptoms of a pec major sprain include a sudden sharp pain at the front of the upper arm, near the shoulder and depending on the grade of muscle strain, swelling (haematoma) of the front of the shoulder and upper arm. Tests which reproduce pain help confirm the diagnosis and include getting the patient to pull their arm across the front of the chest or rotate it inwards against resistance. A visible gap or lump in the muscle may appear.
The Latissimus dorsi muscle or ‘lats’ is another large, flat “V” shaped muscle of the torso. It spans the width of your back and helps control the movement of your shoulders and is often referred as the “climbers” muscle. With a Latissimus dorsi strain, you might feel pain in your low back, mid-to-upper back, along the base of your scapula or shoulder blade, or in the back of the shoulder. You may even feel pain along the inside of the arm, all the way down to your fingers.
The Serratus anterior muscle spans the upper eight or nine ribs. This muscle helps you rotate or move your scapula or shoulder blade forward and up. Sometimes it’s referred to as the “boxer’s muscle,” since it’s responsible for the movement of the scapula when a person throws a punch. Serratus muscle strain typically from repetitive activities such as tennis results in pain in the chest, back, or arm and can make it difficult to lift your arm overhead or have a normal range of motion with the arm and shoulder. It can also be associated with arm or finger pain, difficulty with deep breathing and shoulder blade pain. Serratus anterior myofascial pain syndrome is part of a broader set of conditions known as myofascial pain syndromes. Myofascial pain is a process in which pain and dysfunction are related to the development and persistence of focal sensitive areas or trigger points, that when pressed can cause referred pain (pain felt elsewhere).
Though not strictly a chest wall muscle, the upper Rectus abdominis muscle and External oblique muscle can also be strained, torn or even ruptured leading to pain, which depending on the site of injury can lead to lower chest wall pain and pain when pain twisting from a seated position or when rising from a bed particularly if flexing (bending).
Sternalis syndrome presents with anterior chest pain associated with localised tenderness over the body of the sternum or overlying sternalis muscle; palpation often causes radiation of pain bilaterally. It is an unusual cause of anterior chest wall pain as it appears to be associated with an accessory muscle, the sternalis muscle which is present in only around 5-10% of people and sit in a variable position in front of the main pectoralis muscle. When symptomatic, it is another form of myofascial pain syndrome.
Though uncommon, Stress fractures of the ribs can be seen following repetitive activity or in increased loading. They can occur in the first rib, and less commonly other ribs particularly in those engaged in repetitive forceful sports such as rowers or weightlifters. The pain which is localised to the area with associated tenderness may start gradually but ends to worsen and is only eased with rest and or avoidance of the repetitive activity.
Xiphoid process pain (xiphoidalgia) occurs for varying reasons but is often related to minor trauma to the area or over exercise (such as abdominal crunches). Local inflammation can also occur. See Complex chest wall problems.
Spontaneous subluxation of the sternoclavicular joint is another very specific cause of isolated chest wall pain. See other associated problems.
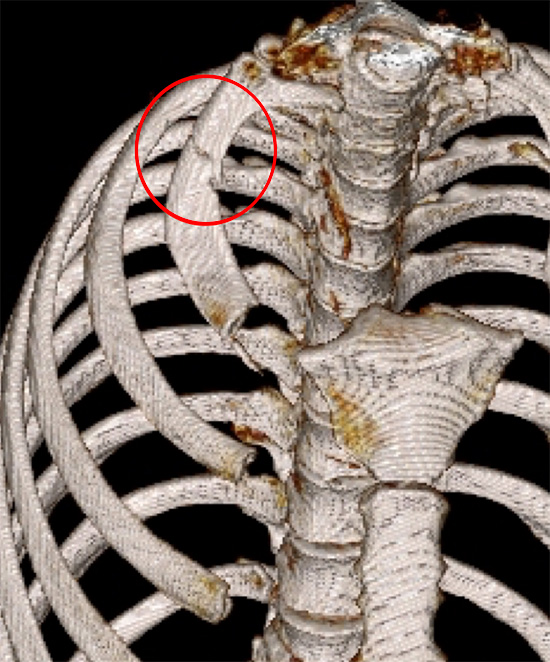
Stress fracture of right first rib (red ring) in a body builder
Arthritic and rheumatological causes of chest wall pain
| Arthritic and Rheumatic diseases causes of chest wall pain | Less Common |
|---|---|
| Fibromyalgia | Sternoclavicular hyperostosis |
| Rheumatoid Arthritis | Systemic lupus erythematous |
| Axial spondylarthritis (including ankylosing spondylitis) | Septic arthritis of the chest wall |
| Osteophytes of the chest (from osteoarthritis or tendonitis) | Relapsing polychondritis |
| Psoriatic arthritis |
Arthritis refers to joint inflammation, the most common is osteoarthritis. Related to arthritis are Rheumatic diseases that are characterized by inflammation that affects the connecting or supporting structures of the body — most commonly the joints, but also sometimes the tendons, ligaments, bones, and muscles. Rheumatic diseases that primarily affect the spine are considered spondyloarthropathies such as ankylosing spondylitis. See other associated problems.
Fibromyalgia is a long-term condition that causes pain and tenderness all over your body. When it extends to the chest, the pain feels like an intense stabbing sensation primarily in the centre of the chest, around the breastbone and rib cage. It’s thought to be caused by your nervous system not being able to control or process pain signals from other parts of your body. The condition is also linked to increased sensitivity to pain, headaches. extreme tiredness (fatigue), muscle stiffness, difficulty sleeping problems with mental processes such as problems with memory and concentration. There is no specific diagnostic test.
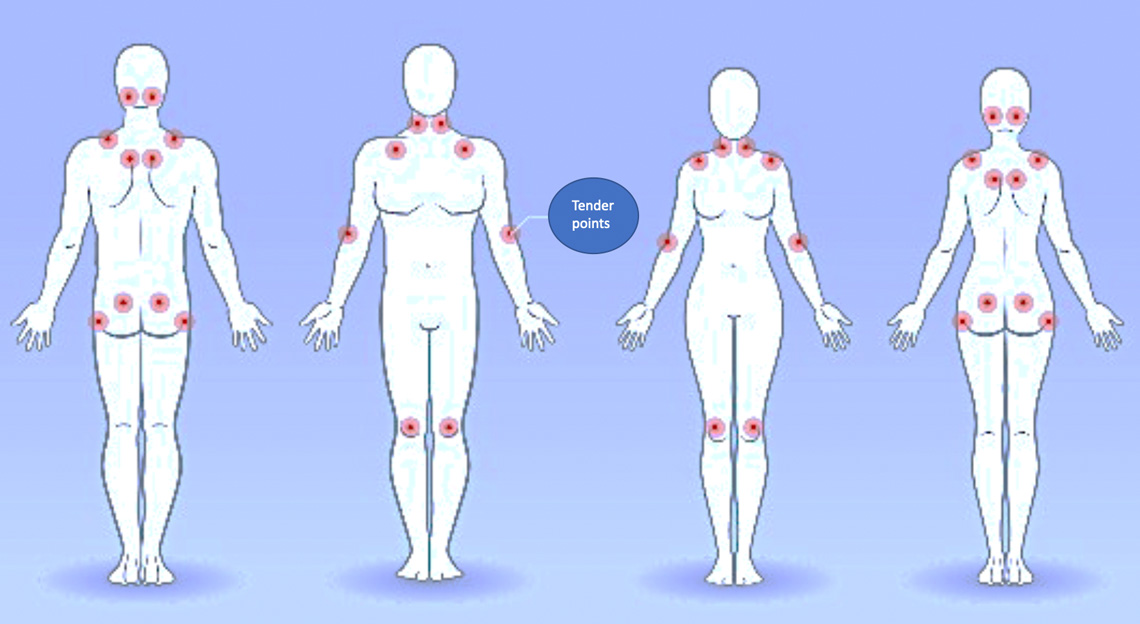
Fibromyalgia and the associated paired tender points
A bone spur (osteophyte) is a tiny pointed outgrowth of bone. Bone spurs are usually caused by local inflammation, such as from degenerative arthritis (osteoarthritis) or tendonitis. Bone spurs develop in areas of inflammation or injury of nearby cartilage or tendons. Bone spurs may or may not cause symptoms.

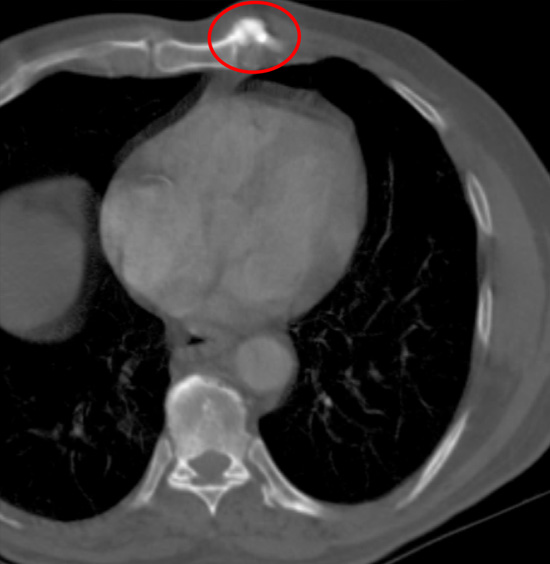
Osteophyte of the sternum (red ring). It was excised with relieve of pain
Systemic diseases can cause chest wall pain. Sternocostoclavicular hyperostosis is a chronic inflammatory disorder which presents with erythema, swelling, and pain of the sternoclavicular joint. See other associated problems. Other conditions such as systemic lupus erythematosus, or SLE can cause chest pain on deep breathing. When this pain is not caused by pleurisy (inflammation of the lining of the chest cavity), it is commonly caused by inflammation of the chest muscle, cartilage, or ligaments, or of the joints that connect the ribs to the breastbone (costochondral joints). Septic arthritis of the sternoclavicular joint is an unusual infection, that can lead to chest wall pain. See other associated problems. Relapsing polychondritis is an immune-mediated systemic disease characterized by recurrent episodes of inflammation of cartilaginous and proteoglycan-rich tissues. It typically affects the cartilage of the ears and nose but potentially all types of cartilage may be involved including rarely the costal cartilage, so is a rare cause of chest wall pain.
Generalised causes of isolated chest wall pain
Several ‘generalised’ conditions can cause symptoms of localised chest wall pain. A sinister cause of local chest wall pain and tenderness is a Pathological fracture. A pathologic fracture is a broken bone such as a rib, that's caused by a disease, rather than an injury. Some conditions weaken your bones, which makes them more likely to break. Conditions that can cause pathological fractures including osteoporosis, osteomalacia, Paget's disease, osteitis, osteogenesis imperfecta, benign bone tumours and cysts, secondary malignant bone tumours and primary malignant bone tumours. See Chest wall lumps. Everyday things, such as coughing, twisting suddenly or bending over can fracture a rib that's been weakened by one’s of these conditions.
Non-chest wall related causes of chest pain
There are many other causes of apparent chest wall pain, and that is why a through clinical history and clinical examination is important including a medical history and assessment for risk factors for heart, lung and gastrointestinal disease. Further tests may aid diagnosis.
Non-chest wall related causes of chest pain
 |
Angina Myocardial Infarction (heart attack) Pericarditis (inflammation of pericardial sac) Myocarditis (inflammation of heart muscle) |
 |
Pneumonia (chest infection) Pleurisy (inflammation of pleural lining) Pulmonary embolism (blood clot to lung) |
 |
Oesophagitis or Gastroesophageal Reflux (Heartburn) Oesophageal Spasm (swallowing difficulties) Peptic ulcer (stomach ulcer) Gallbladder (gallstones) Pancreatitis (inflammation of the pancreas) |
Treatment
Depends on the overlying cause, most often particularly in adults it is what is called a ‘diagnosis of exclusion’ (looking for sinister causes of chest pain, such as cardiac related pain and if excluded labelling chest wall pain as musculoskeletal). For many types of Musculoskeletal causes of isolated chest wall pain the treatment options are similar. See Treatments.
| Treatment options for isolated musculoskeletal chest wall pain |
|---|
| Reassurance & explanation of diagnosis |
| Avoidance of aggravating activities & restriction of certain activities |
| Passive thoracic mobility exercises (stretching) |
| Application of heat for muscle soreness / spasm or cold for swelling |
| Simple analgesia (see Treatment) |
| If symptoms persist, consider physiotherapy assessment & treatment. May include biomechanical assessment with targeted stretching and strengthening exercises, mobilization & soft tissue therapy |
| Trigger point injections of local anaesthetic +/- corticosteroid (see Trigger Point, Peripheral nerve and Joint Injections) |
For specific causes of chest wall pain, once the diagnosis is established additional treatments such as targeted physiotherapy and sports medicine techniques including therapeutic ultrasound or infrared, Platelet-Rich Plasma Injections, surgical options and drugs to modulate the symptoms of arthritis or rheumatic diseases may be appropriate.